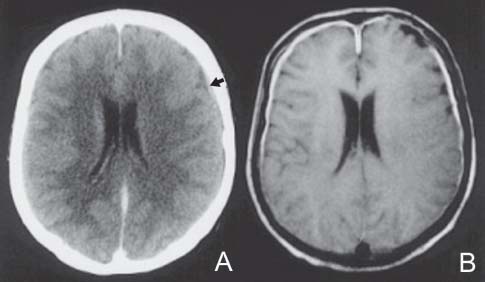
Case 19 Meningeal Carcinomatosis Ramez Malak and Robert Moumdjian Fig. 19.1 (A) Computed tomography scan of the brain and (B) T1-weighted axial magnetic resonance image of the brain, both with contrast. Arrow in (A) points to contrast enhancement of the meninges. Fig. 19.2 T2-weighted magnetic resonance image of the lumbar spine, midsagittal sec tion. MRI of the lumbar spine (Fig. 19.2) shows multiple metastases along the cauda equina.

 Clinical Presentation
Clinical Presentation
 Questions
Questions
 Answers
Answers
19 Meningeal Carcinomatosis
Case 19 Meningeal Carcinomatosis Fig. 19.1 (A) Computed tomography scan of the brain and (B) T1-weighted axial magnetic resonance image of the brain, both with contrast. Arrow in (A) points to contrast enhancement of the meninges. Fig. 19.2 T2-weighted magnetic resonance image of the lumbar spine, midsagittal sec tion.
Clinical Presentation
Questions
Answers
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


