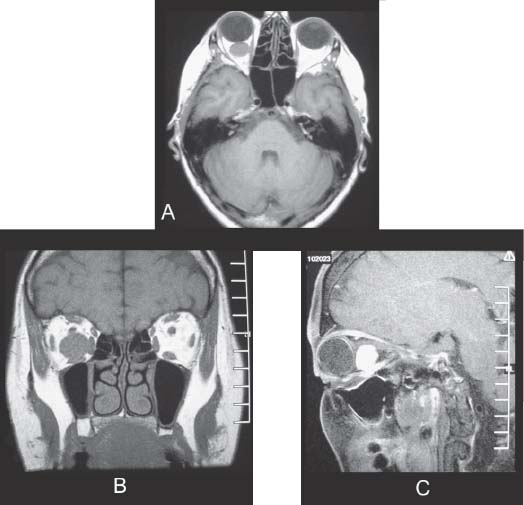
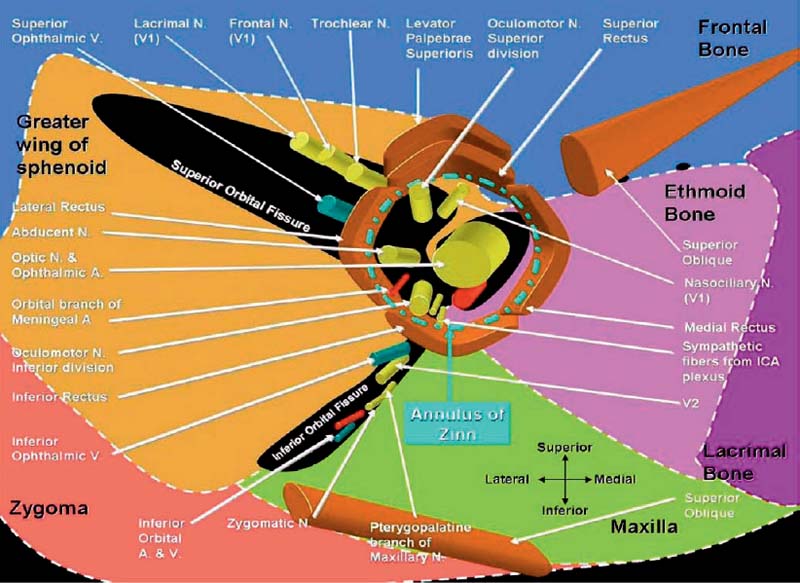
Case 23 Orbital Tumor Fig. 23.1 (A) Axial T1-weighted, (B) coronal T1-weighted, and (C) sagittal T1-weighted magnetic resonance images (MRIs) of the brain with gadolinium contrast brought by the patient during the initial visit. Fig. 23.2 Artist’s rendering of the content of the annulus of Zinn.
 Clinical Presentation
Clinical Presentation
 Questions
Questions
 Answers
Answers
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue



