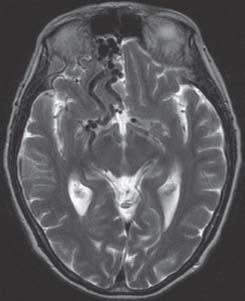
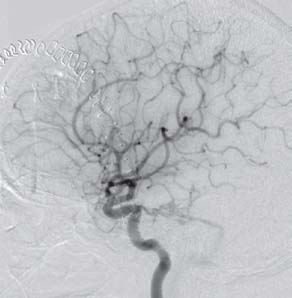
Case 27 Dural Arteriovenous Fistula Fig. 27.1 Axial T2-weighted magnetic resonance image of the head. Fig. 27.2 Digital subtraction angiography lateral view, right carotid injection. Fig. 27.3 Digital subtraction angiography postoperative lateral view, right carotid injection.

 Clinical Presentation
Clinical Presentation
 Questions
Questions
 Answers
Answers
< div class='tao-gold-member'>
27 Dural Arteriovenous Fistula
Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


