Case 35 Concomitant Arteriovenous Malformation and Aneurysm
Julius July and Eka Julianta Wahjoepramono
Fig. 35.1 Plain axial computed tomography scan of the head.
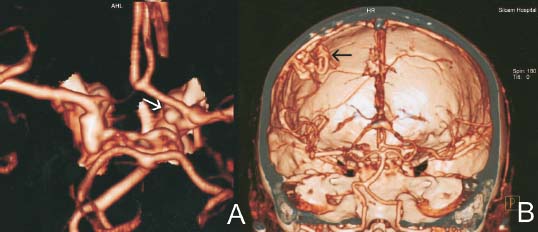
Fig. 35.2 Three-dimensional reconstructed computed tomography angiogram showing (A) aneur ysm (white arrow) and (B) ar teriovenous malformation (black arrow).
- A 50-year-old man with past medical history of hypertension and heavy smoking presented to the ER with sudden onset left partial ptosis.
- Ten days prior, he had a very severe headache and was admitted to another hospital for 3 days and was sent home without imaging studies of his head or lumbar puncture.
- Physical examination reveals that he is fully oriented with moderate headache. He has a left partial ptosis and a left dilated pupil (5 mm, compare with the right, 3 mm) and is less reactive to the light. The remainder of the neurologic examination is normal.
- Initial plain computed tomography (CT) scan is shown in Fig. 35.1.
Fig. 35.3 Postoperative computed tomography scan of the head performed after neurologic deterioration. Sequential images showing (A) basilar cisterns, (B) cour se of ventriculostomy, and (C) site of resection of arteriovenous malformation.
< div class='tao-gold-member'>
 Clinical Presentation
Clinical Presentation Questions
Questions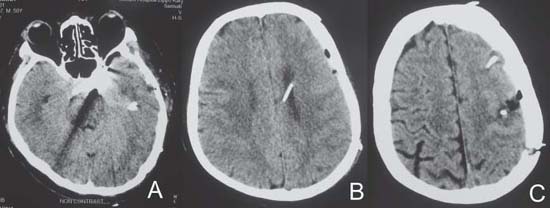
 Answers
Answers


