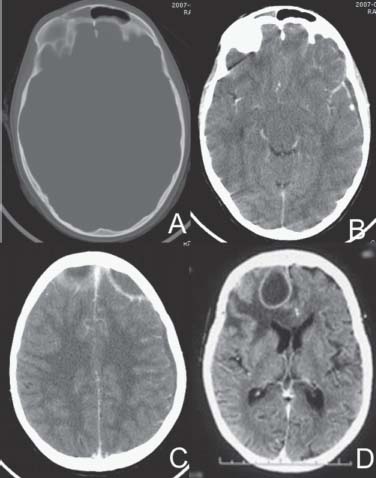
Case 64 Frontal Abscess with Sinus Involvement Ramez Malak and Rober t Moumdjian Fig. 64.1 Computed tomography scan of the brain with (A) bone windows and (B–D) brain windows contrast enhanced.
 Clinical Presentation
Clinical Presentation
 Questions
Questions
 Answers
Answers
64 Frontal Abscess with Sinus Involvement
Case 64 Frontal Abscess with Sinus Involvement Fig. 64.1 Computed tomography scan of the brain with (A) bone windows and (B–D) brain windows contrast enhanced.
Clinical Presentation
Questions
Answers
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


