Figure 13-1 Magnetic resonance imaging scan of the lumbosacral spine. Top: Midsagittal view of lumbosacral spine with T2 (left) and T1 with gadolinium contrast (right) sequences. Arrows highlight enlarged roots with gadolinium enhancement. Bottom: Transverse sections through cauda equina with T2 (left) and T1 with gadolinium contrast (right) sequences. Arrows highlight lumbar root clumping with gadolinium enhancement.
Because several treatable etiologies were under consideration, a posterior lumbar rootlet biopsy was performed (Fig. 13-2), which revealed metastatic lobular breast adenocarcinoma. The tumor cells often tracked along the perineurium and endoneurial septae in a single file manner. The abnormal cells stained positive for cytokeratin-7 (CK-7) and negative for CK-20. Hormonal staining was positive for estrogen receptor and negative for progesterone receptor and human epidermal growth factor receptor 2.
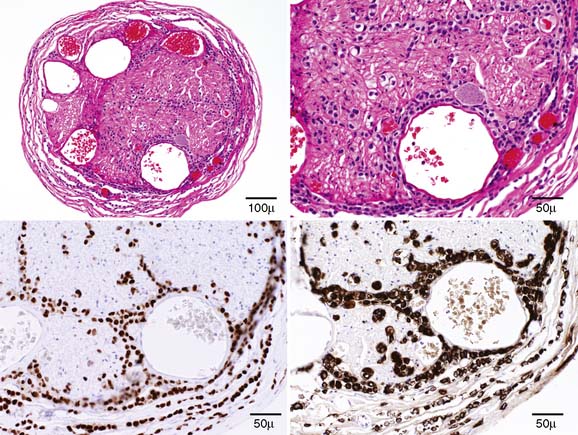
Figure 13-2 Histopathology of lumbar posterior rootlet. Transverse section of hematoxylin and eosin–stained lumbar rootlet at low (top left) and high (top right) power. Note cells with large nuclei insinuating single file throughout nerve tissue. Immunostaining with estrogen receptor (bottom left) and cytokeratin-7 (bottom right) epitopes help confirm diagnosis of metastatic lobular breast adenocarcinoma.
Interestingly, the patient had no history of breast cancer and, in fact, had a normal mammogram 3 months before the onset of neurologic symptoms. Further oncologic work-up ensued, which included a normal breast examination, mammogram, and breast ultrasound. MRI of the breast revealed a 0.7-cm lobulated mass against pectoral fascia in outer quadrant of right breast. The patient was started on the aromatase inhibitor letrozole, and prednisone was tapered off.
Related posts:
 Malignant Peripheral Nerve Sheath Tumor
Borrelia Neuropathy with Necrotizing Vasculitis
Adrenomyeloneuropathy Masquerading as Charcot-Marie-Tooth Disease
Focal Mononeuropathy Onset of Amyotrophic Lateral Sclerosis
A Case of Guillain-Barré Syndrome Associated with Anti-GD1b Immunoglobulin G Antibodies
Length-Related Axonal Loss in Neuropathy
Malignant Peripheral Nerve Sheath Tumor
Borrelia Neuropathy with Necrotizing Vasculitis
Adrenomyeloneuropathy Masquerading as Charcot-Marie-Tooth Disease
Focal Mononeuropathy Onset of Amyotrophic Lateral Sclerosis
A Case of Guillain-Barré Syndrome Associated with Anti-GD1b Immunoglobulin G Antibodies
Length-Related Axonal Loss in Neuropathy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


