Fig. 26.1
(a, b) T2-weighted axial MRI scans revealing a small and a large arachnoid cyst located at the cerebellopontine angle
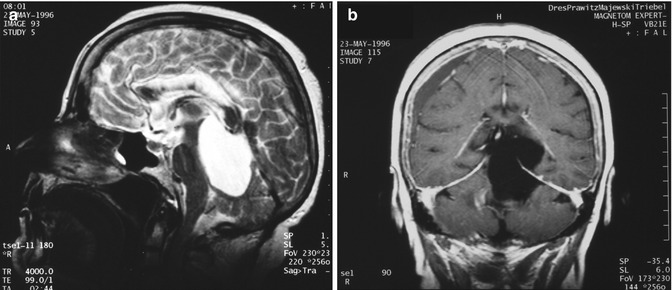
Fig. 26.2
T1- and T2-weighted gadolinium-enhanced images (a, b) displaying a huge arachnoid cyst located dorsally to the brainstem, mainly at the posterior fossa and partially extending into the middle fossa. Sagittal and coronal images show the important dorsal compression of the brainstem and supratentorial extension of the lesion through the tentorial notch
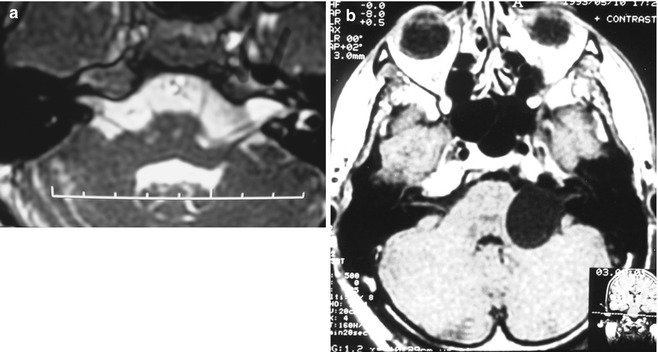
Fig. 26.3
(a) T2-weighted axial MRI scan showing an arachnoid cyst located inside of the internal auditory canal. (b) Axial T1-weighted MRI scan showing an arachnoid cyst located in the CPA, extending into the internal auditory canal, with the same signal intensity as the CSF, compressing the brainstem
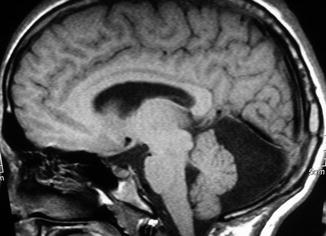
Fig. 26.4
T1-weighted sagittal MRI displaying an arachnoid cyst located posterior to the cerebellum
26.5 Surgical Treatment of AC
The indication for surgery and the mode of surgical treatment are still a matter of debate [7, 12, 13, 39]. In many cases, AC are asymptomatic and do not grow progressively. Conservative management with regular radiological control will identify those cases with gradual cyst enlargement that need surgical treatment. Surgical indication and technique should be based on the following criteria: (1) type of AC (communicating or noncommunicating cyst), (2) growth of the cyst, (3) compression or displacement of the surrounding neurovascular structures and, most importantly (4), patient’s symptoms and signs, and especially ongoing clinical worsening.
Different types of surgical approaches can be performed [3, 7, 13]. Cyst fenestration, stereotactic punction, endoscopic cyst fenestration, cystoperitoneal shunt, cyst marsupialisation into the subarachnoid space and complete or partial resection of the cyst wall are the main options [7, 10, 17, 40]. Advantages and disadvantages of each surgical treatment have been extensively discussed [7, 32]. Among the most frequently used techniques are aspiration techniques like stereotactic punction or endoscopic punction. Reclosure of the cyst wall or insufficient fenestration and therefore inadequate drainage into the subarachnoid space are the main reasons for recurrence and regrowth. Cystoperitoneal shunting also carries a considerable rate of obstruction and/or recurrence. Nevertheless, cyst shunting presents good results with the small ratio of recurrence for AC located in the middle fossa associated with hydrocephalus [6, 7, 30, 32].
In our experience, the most likely prevention of cyst recurrence is open surgery with resection of the entire cyst wall especially for AC located at the posterior fossa. Because of the close cyst relationship to many important neurovascular structures in this area, e.g. brainstem and 4th to 12th cranial nerves, cyst shunting, punction or endoscopic procedures may be hazardous in these cases.
Patients with posterior fossa AC with compression of the brainstem or surrounding neurovascular structures and correlating symptoms will usually profit from the surgical treatment. Suboccipital craniotomy permits a good and safe exposure of the cyst and surrounding neurovascular structures. Radical resection of the cyst and careful resection of the cyst parts adherent to vessels and cranial nerves minimise the chance of recurrence. Furthermore, patients with additional vascular compression syndromes, as in one of our cases, will more likely improve by open surgery, wide cyst resection and, if necessary, microsurgical vascular decompression as well.
In some particular cases, strong adhesion between the cyst wall and the neurovascular structures may be found. A trial of radical removal of the cyst wall, in such cases, may result in postoperative cranial nerves deficits, e.g. facial palsy, hearing loss and swallowing disturbance. Extensive resection and wide opening of the cyst without direct manipulation of the surrounding cranial nerves will provide considerable connection of the AC to the cisterns and will avoid such postoperative morbidity. Regular follow-up on such cases is especially indicated in order to detect a possible recurrence.
In cases of posterior fossa communicating AC with associated hydrocephalus, ventriculoperitoneal shunting should be first attempted. If no relief of the preoperative symptoms is achieved and serial postoperative scans demonstrate no shrinking of the cyst, open surgery should be performed.
Around 50 cases of posterior fossa AC with CPA involvement have been reported in the literature. All these cases were treated according to different treatment protocols. Therefore, the rate of recurrence, regrowth and clear decision-making concerning the best surgical technique are still unclear.
Samii M, Carvalho GA et al. published, in 1999, a report of 12 patients that underwent surgery upon of arachnoid cysts involving the posterior fossa and displayed 7 cases of AC that were located within the cerebellopontine angle (CPA), 3 cases in the CPA with major extension dorsal to the brainstem and 2 cases at the CPA extending into the internal auditory canal [28]. A suboccipital retrosigmoid approach was performed in all patients. Radical resection of the cyst could be accomplished in all but one cases. There was no mortality. Major postoperative morbidity was present in one case due to intraoperative air embolism in the semisitting position and strong adherence of the cyst wall with the surrounding neurovascular structures. Short- and long-term follow-up (over 3.3 years) displayed improvement of most preoperative symptoms. Suboccipital approach showed to provide a good and safe exposure of vascular structures and cranial nerves in the CPA. Complete resection with few exceptions is obviously tolerated very well, as demonstrated by our series (Fig. 26.5). This underlines the chances and advantages of this concept.
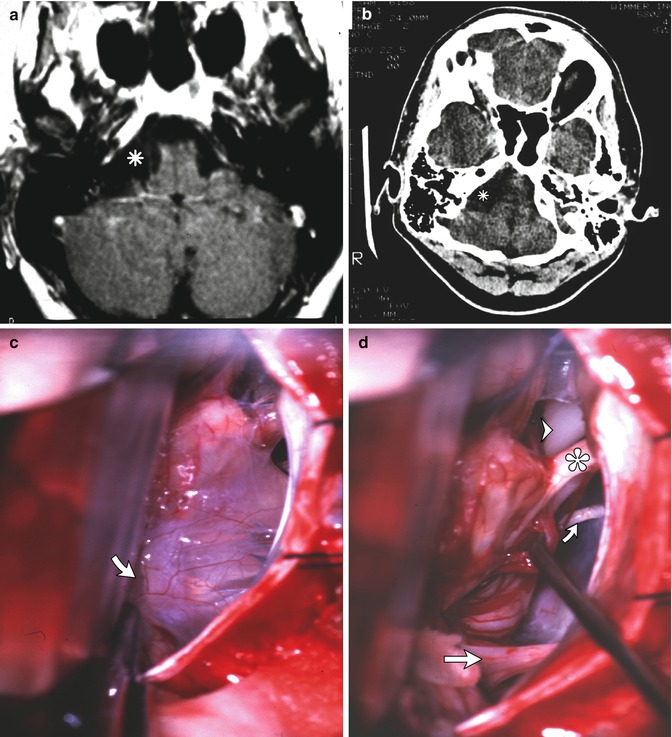
Fig. 26.5
(a, b) Axial T1-weighted MRI picture after gadolinium and axial CT scan displaying the AC at the CPA, compressing the brainstem. (c) After a lateral suboccipital retrosigmoid approach and retraction of the cerebellum, the AC (arrow) at the CPA can be displayed covering and surrounding the cranial nerves. (d) After careful radical removal of the AC, the trigeminal nerve (arrowhead), abducens nerve (upward arrow), facial-cochlear nerve complex and caudal cranial nerves (arrow) can be well recognised
26.6 Conclusion
Microsurgical treatment of arachnoid cysts located in the posterior fossa is usually beneficial. Good exposure of the vascular and cranial nerve structures in the cerebellopontine angle is essential for a safe removal of these cysts. The suboccipital approach allows a radical resection of most cysts without hazarding the surrounding structures and reducing the chance of cyst recurrence.
Complete cyst resection is the most reliable option for prevention of recurrence. The fact that it is so well tolerated provides the best reason for application of this mode of treatment. Long-term follow-up displays the improvement of the majority of the preoperative symptoms.
References
1.
Becker T, Wagner M, Hofmann E et al (1991) Do arachnoid cysts grow? A retrospective CT volumetric study. Neuroradiology 33:341–345PubMedCrossRef
Related posts:
 Preoperative Visualization of the Facial Nerve Using Diffusion Tensor Imaging Fibre Tracking in Patients with Large Vestibular Schwannomas
Considerations for Experimental Neuromodulation Following Grafting of the Spinal Cord to Skeletal Muscles for Clinical Application
Chordomas and Chondrosarcomas
Preservation of the Olfactory Tract in Bifrontal Craniotomy
The Surgical Management of Trigeminal Schwannomas
Bypass and Vascular Reconstruction for Posterior Circulation Aneurysms
Preoperative Visualization of the Facial Nerve Using Diffusion Tensor Imaging Fibre Tracking in Patients with Large Vestibular Schwannomas
Considerations for Experimental Neuromodulation Following Grafting of the Spinal Cord to Skeletal Muscles for Clinical Application
Chordomas and Chondrosarcomas
Preservation of the Olfactory Tract in Bifrontal Craniotomy
The Surgical Management of Trigeminal Schwannomas
Bypass and Vascular Reconstruction for Posterior Circulation Aneurysms
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


