Brain Edema and Disorders of Intracranial Pressure
Brain Edema and Disorders of Intracranial Pressure
Stephan A. Mayer
INTRODUCTION
Brain edema accompanies a wide variety of pathologic processes. It plays a major role in head injury, stroke, brain tumor, and cerebral infections such as brain abscess, encephalitis, and meningitis. Less common but equally devastating causes of brain edema include fulminant hepatic encephalopathy, hypertensive encephalopathy and posterior reversible encephalopathy syndrome (PRES), hydrocephalus, hypoxic-ischemic injury, hyponatremia, and other disorders associated with acute hypo-osmolality (Table 107.1). Brain edema occurs in many different forms; clearly, it is not a single pathologic or clinical entity.
BRAIN EDEMA
Brain edema is defined as an increase in brain volume caused by an increase in water and sodium content. When well localized or mild in degree, brain edema is associated with little or no clinical evidence of brain dysfunction; however, when severe, it can cause massive intracranial mass effect and potentially fatal brain stem herniation. Because the brain is encased in a rigid cranial vault, focal or generalized brain edema results in intracranial hypertension when it is severe enough to exceed the compensatory mechanisms that modulate intracranial pressure (ICP).
TABLE 107.1 Conditions Characterized by Brain Edema
Intracellular Edema
Cytotoxic
Cerebral infarction
Hypoxic-ischemic injury
Reye syndrome
Osmotic
Acute hyponatremia
Diabetic ketoacidosis
Dialysis dysequilibrium syndrome
Extracellular Edema
Vasogenic
Brain tumor
Abscess
Postendarterectomy hyperperfusion syndrome
High-altitude cerebral edema
Acute intermittent porphyria
MS
Posterior reversible encephalopathy syndrome
Hypertensive encephalopathy
Eclampsia
Lead encephalopathy
Immunosuppressants (tacrolimus/FK-506, cyclosporine A, interferon alpha [IFN-α]), intravenous immunoglobulin (IVIG)
Chemotherapeutic agents (cisplatin, cytarabine)
Erythropoietin
End-stage renal disease
Interstitial
Hydrocephalus
Combined Intracellular and Extracellular Edema
Vasogenic and cytotoxic
Intracerebral hemorrhage
Subarachnoid hemorrhage
Dural sinus thrombosis
Traumatic brain injury
Encephalitis
Meningitis
Hepatic encephalopathy
MS, multiple sclerosis.
Brain tissue shifting or herniation results from the generation of compartmentalized mass effect and ICP gradients within the skull. The major forms of herniation are central, transtentorial (or uncal), subfalcine (or cingulate), and cerebellar (see Fig. 18.5). Brain edema and vascular engorgement are different processes.
Brain engorgement is an increase in the blood volume of the brain caused by obstruction of the cerebral veins and venous sinuses or by arterial vasodilatation, such as that caused by hypercapnia. Hypertension severe enough to overwhelm the brain’s capacity to autoregulate and maintain a constant level of cerebral blood flow (CBF) is another common cause of brain engorgement. Brain engorgement is also known as hyperemia or luxury perfusion.
PATHOBIOLOGY
Brain edema has conventionally been classified into three major categories: vasogenic, cytotoxic, and interstitial. The basic features of these three forms of cerebral edema are summarized in Table 107.2 with regard to pathogenesis, location and composition of the edema fluid, and changes in capillary permeability. A newer classification scheme focuses on the primary location of the edema fluid as intracellular or extracellular. In this scheme, the two main forms of intracellular edema are cytotoxic and osmotic, and the two main forms of extracellular edema are vasogenic and interstitial (hydrocephalic). Many causes of brain edema, including hemorrhagic stroke, venous infarction, and trauma, lead to a combination of these different forms of brain edema, and the varying contributions of each form of edema may change over time.
TABLE 107.2 Classification of Brain Edema
Vasogenic
Cellular
Interstitial
Pathogenesis
Increased capillary permeability
Cellular swelling caused by energy failure or osmotic forces
Increased brain fluid due to block of CSF absorption
Effectiveness limited by blood-brain barrier disruption
Effective
Rarely useful
CSF, cerebrospinal fluid.
Modified from Fishman RA. Brain edema. In: Fishman RA, ed. Cerebrospinal Fluid in Diseases of the Nervous System. 2nd ed. Philadelphia: WB Saunders, 1992:116-137.
Vasogenic Edema
Vasogenic edema is a form of extracellular edema characterized by increased permeability of the blood-brain barrier to fluid, solutes, and macromolecules such as the plasma proteins, whose entry is normally limited by tight junctions between the capillary endothelial cells. The increase in permeability is visualized when contrast enhancement is observed with computed tomography (CT) or magnetic resonance imaging (MRI). Increased cerebrospinal fluid (CSF) protein levels are also indicative of increased endothelial permeability. MRI fluid-attenuated inversion recovery (FLAIR) sequences are more sensitive than CT for demonstrating the increases in brain tissue water content and extracellular volume that characterize vasogenic edema.
The biochemical basis of the changes in membrane integrity that underlie vasogenic edema involves the effects of free radicals (i.e., superoxide ions, hydroxyl radicals, singlet oxygen, and nitric oxide) and polyunsaturated fatty acids, most notably arachidonic acid, in the peroxidation of membrane phospholipids. The ability of glucocorticoids to inhibit the release of arachidonic acid from cell membranes may explain their beneficial effects in vasogenic edema. By contrast, steroids such as dexamethasone have not been shown to be therapeutically useful in the treatment of cytotoxic edema or vasogenic brain edema associated with stroke or trauma.
Vasogenic edema is characteristic of clinical disorders in which a local tissue inflammatory response occurs when angiogenesis is stimulated by neoplasm or when severe hypertension overwhelms the brain’s capacity to autoregulate CBF. These disorders include brain tumor, abscess, hemorrhage, infarction with reperfusion, hypertensive encephalopathy, and traumatic contusion. Vasogenic edema related to varying degrees of vasodilation and blood-brain barrier disruption is also seen with acute demyelinating lesions in multiple sclerosis, hepatic or lead encephalopathy, Reye syndrome, and meningitis or encephalitis. Functional manifestations of vasogenic edema include focal neurologic deficits, focal electroencephalogram (EEG) slowing, disturbances of consciousness, and severe intracranial hypertension. In patients with brain tumor, whether primary or metastatic, the clinical signs are often caused more by the surrounding edema than by the tumor mass itself.
Cytotoxic (Osmotic) Edema
Cytotoxic edema is characterized by swelling of all the cellular elements of the brain (neurons, glia, and endothelial cells) with a concomitant reduction in the volume of the extracellular fluid space of the brain. Capillary permeability is usually not affected by osmotic edema (i.e., hyponatremia) or in the early phase of a hypoxic-ischemic insult. The biologic basis of cytotoxic or osmotic brain edema involves astrocytic calcium signaling and activation of aquaporin-4 channels, which are the major influx route for water into the cell. Patients with pure cytotoxic edema have a normal CSF protein, and CT and MRI do not reveal contrast enhancement. MRI diffusion-weighted imaging (DWI) reflects the restricted diffusion of water within swollen cells and is by far the most sensitive method for imaging cytotoxic edema (see also Chapter 21).
There are several causes of cytotoxic or osmotic edema, the most important being hypoxia-ischemia, acute hypo-osmolality of the plasma relative to the intracellular compartment, and the osmotic dysequilibrium syndromes. Hypoxia after cardiac arrest or asphyxia results in cerebral energy depletion. The cellular swelling is determined by the appearance of increased intracellular osmoles (especially sodium, lactate, and hydrogen ions) that induce the rapid entry of water into cells. Cytotoxic edema also plays a large role in the tissue swelling that occurs after cerebral infarction. Acute hypo-osmolality of the plasma and extracellular fluid is caused by acute dilutional hyponatremia, syndrome of inappropriate secretion of antidiuretic hormone (SIADH), or severe sodium depletion (see also Chapter 12). Osmotic dysequilibrium syndromes occur with hemodialysis or diabetic ketoacidosis, in which excessive brain intracellular solutes result in excessive cellular hydration when the plasma osmolality is rapidly normalized with therapy. In the case of renal failure, the intracellular solutes presumably include a number of organic acids recovered in the dialysis bath. In diabetic ketoacidosis, the intracellular solutes include glucose and ketone bodies; however, there are also unidentified, osmotically active, intracellular solutes termed idiogenic osmoles that favor cellular swelling.
Major changes in cerebral function can result from processes that result in cytotoxic edema, including encephalopathy, stupor or coma, ICP elevation, brain stem herniation, asterixis, myoclonus, and focal or generalized seizures. As a general rule, intracellular edema caused by osmotic derangements is much more treatable than cytotoxic edema resulting from hypoxic-ischemic injury because cellular function remains viable. The extent of cellular swelling and neurologic dysfunction resulting from acute hypo-osmolality is directly related with how quickly it develops; chronic states of extreme hypo-osmolality that are reached gradually lead to minimal symptomatology. Hypoxic-ischemic injury causes cytotoxic edema and selective cellular necrosis. If the process progresses to frank tissue infarction, vasogenic edema follows. The delay in visualizing contrast enhancement with CT following an ischemic stroke illustrates that time is needed for defects in endothelial cell permeability to develop.
Interstitial (Hydrocephalic) Edema
Interstitial edema is the third type of edema best characterized in obstructive hydrocephalus, in which the water and sodium content of the periventricular white matter is increased because of the movement of CSF across the ventricular ependymal surface. Obstruction of the CSF outflow results in the transependymal movement of CSF and thereby an absolute increase in the volume of the extracellular fluid of the brain. Interstitial edema thus is strictly periventricular on CT and MRI, with predominance at the anterior and posterior aspects of the lateral ventricles. The composition of interstitial edema is similar to CSF. The clinical manifestations of interstitial edema (dementia, psychomotor slowing, and gait disorder) are often difficult to separate from those seen with normal pressure hydrocephalus in which there is physical traction on the periventricular white matter fiber tracts.
SELECTED CAUSES OF BRAIN EDEMA
Cerebral Infarction
Most patients with arterial occlusion initially have cytotoxic edema followed by vasogenic edema, which are together termed ischemic brain edema. The cytotoxic phase takes place over minutes to hours and may be reversible. At this point, DWI may show dramatic changes well before evidence of completed tissue infarction can be demonstrated on MRI FLAIR sequences or by CT. Although osmotic or vasogenic edema can also be DWI positive, a phenomenon called T2 shine through, cytotoxic edema can be further differentiated from these causes on MRI because it is always associated with a reduction (low signal) in the apparent diffusion coefficient (ADC) of water. The vasogenic phase of infarction takes place over hours to days as the tissue swells; in many cases, spontaneous vessel recanalization may occur and accelerate this process. A patchy and heterogenous pattern of contrast enhancement on CT or MRI at this point is characteristic. Despite the theoretical concern that osmotic therapy with mannitol or hypertonic saline may aggravate tissue edema because these osmotically active substances may leak through disrupted endothelial cells into the infarcted brain tissue, clinical experience indicates that these treatments can effectively reverse the early stages of brain stem herniation. Hemicraniectomy is the definitive treatment of choice for younger patients (younger than 60 years) who are at risk for brain stem herniation due to complete infarction of the middle cerebral artery territory (see also Chapter 35).
Intracerebral Hemorrhage
Perihematomal brain edema is a form of vasogenic edema that progressively increases over the first week after intracerebral hemorrhage (ICH, see also Chapter 38). Symptomatic mass effect related to edema formation is the major cause of delayed neurologic deterioration after ICH. Perihematomal edema is caused by the local infiltration of plasma rich in thrombin and other coagulation proteins into the surrounding brain tissue. The thrombin then triggers a unique form of neuro-hemo-inflammation, stimulating the surrounding tissue to produce prostaglandins, complement, leukotrienes, and other inflammatory mediators that promote apoptotic cell death and blood-brain barrier disruption. Dexamethasone is not effective for treating perihematomal edema [Level 1].1 By contrast, large doses of 20% mannitol (1.4 g/kg) have been shown to effectively reduce ICP and reverse clinical brain stem herniation in uncontrolled cohort studies.
Subarachnoid Hemorrhage
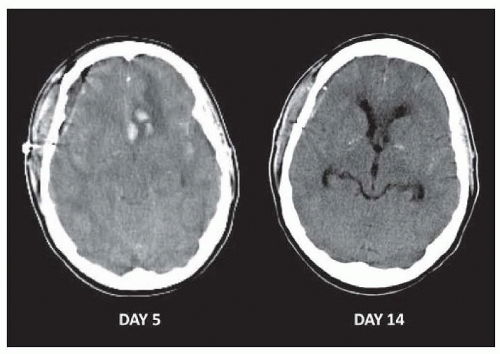
Subarachnoid hemorrhage (SAH, see also Chapter 39) can cause global cerebral edema that typically occurs at onset in poor-grade patients, as well as a variety of forms of focal edema related to focal hematoma formation, cerebral infarction, brain retraction injury, and other causes. The global brain edema is mostly vasogenic in nature (Fig. 107.1). The pathophysiology is thought to reflect transient hypoperfusion as a brief period of intracranial circulatory arrest associated with a massive surge in ICP, followed by reperfusion injury of the brain, with reflex hypertension in the setting of impaired autoregulation causing vascular engorgement. Global cerebral edema on CT affects 20% of patients and is associated with increased mortality and poor functional and cognitive outcome after SAH. Placement of an external ventricular drain is the first step in attaining ICP control; hypertonic saline and hypothermia are promising but untested potential interventions for mitigating further tissue damage.
FIGURE 107.1 Global cerebral edema in a patient with subarachnoid hemorrhage. Day 5: CT shows global swelling of the brain with effacement of the quadrigeminal cisterns. A focus of hemorrhage with surrounding edema is also evident in the left inferior frontal lobe. The patient was undergoing induced hypertension, which later was felt to be exacerbating brain edema. Day 14: Resolution of global cerebral edema is evident.
Venous Infarction
Venous infarction results from occlusion of the cerebral venous and dural sinuses usually in the setting of dural sinus thrombosis (Chapter 40) or as a complication of a neurosurgical procedure. The result is tissue hypoperfusion with congestion and engorgement of the microcirculation, which results in a combination of cytotoxic and prominent vasogenic edema. Imaging shows extensive mass effect, patchy enhancement, and secondary hemorrhagic transformation of the infarct in most cases. In addition to standard measures to control ICP, treatment is directed at preventing clot propagation within the venous system with heparin anticoagulation. Interventional approaches to restore venous flow with local thrombolytic therapy can also be attempted as a heroic measure.
Only gold members can continue reading. Log In or Register to continue