Fig. 33.1
Cavernous sinus cavernous hemangioma. (a) Axial T2-weighted MRI showing a rounded, hyperintense lesion in the left parasellar region and cavernous sinus. (b) Axial T1-weighted MRI shows the same lesion that is isointense to gray matter. (c, d) Axial and coronal contrast-enhanced T1-weighted MRI shows avid contrast enhancement of the left cavernous sinus hemangioma (adapted from Tannouri et al with permission, Neuroradiology. 2001;43:317–320)
33.3 Histopathology
CSCHs are frequently lined by a pseudocapsule. Vascular channels are commonly seen, with intratumoral hemorrhage and calcification being rare findings in CSCHs (Fig. 33.2).
CSCHs can be classified as one of two subtypes [14]:
Type A CSCHs are characterized by adjacent thin-walled, sinusoidal vessels with little intervening connective tissue. These CSCHs are associated with a high degree of intraoperative bleeding.
Type B CSCHs are characterized by more interconnective tissue and fewer sinusoidal vessels. These CSCHs are easier to resect surgically because they are associated with less bleeding.
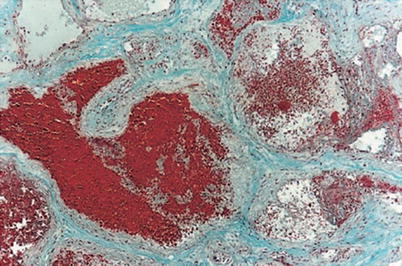
Fig. 33.2
Masson trichrome stain showing a cavernous hemangioma with compact, sclerotic vessels and little interstitium (adapted from Tannouri et al with permission, Neuroradiology. 2001;43:317–320)
33.4 Clinical and Surgical Management
When necessary, surgical resection of a symptomatic cavernous sinus cavernous hemangioma may be performed via an endonasal endoscopic approach or craniotomy [4].
The extradural temporopolar approach to the cavernous sinus is often utilized when open craniotomy is recommended [15].
Injection of fibrin glue has been successfully used to control intraoperative bleeding during resection of CSCHs [16].
Although recurrence rates are low following surgical resection via craniotomy, the incidence of cranial nerve paresis is rather high [2].
References
1.
2.
Goel A, Muzumdar D, Sharma P. Extradural approach for cavernous hemangioma of the cavernous sinus: experience with 13 cases. Neurol Med Chir (Tokyo). 2003;43:112–8; discussion 119.CrossRef
Related posts:
 Neurocysticercosis of the Sellar Region
Arteriovenous Malformations
Neurocysticercosis of the Sellar Region
Arteriovenous Malformations
 Olfactory Neuroblastoma and Sellar Neuroblastoma
Olfactory Neuroblastoma and Sellar Neuroblastoma
 Traumatic Injury of the Sellar Region, Pituitary Stalk Disruption, and Posttraumatic Anosmia
Traumatic Injury of the Sellar Region, Pituitary Stalk Disruption, and Posttraumatic Anosmia
 Schwannomas of the Sellar and Parasellar Region
Schwannomas of the Sellar and Parasellar Region
 Nasopharyngeal Carcinoma and Squamous Cell Carcinoma of the Paranasal Sinuses
Nasopharyngeal Carcinoma and Squamous Cell Carcinoma of the Paranasal Sinuses
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


