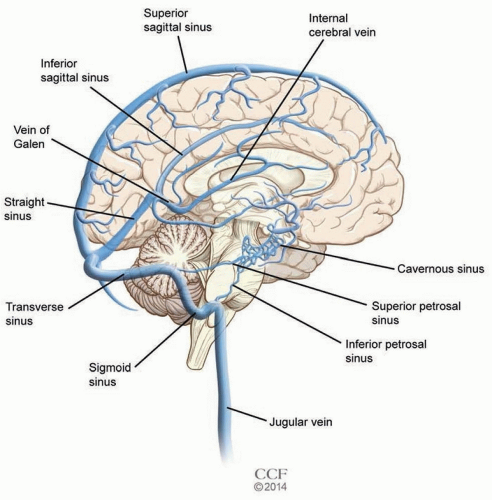
Cerebral venous thrombosis (CVT) is thrombosis of the venous channels that drain blood from the brain (Fig. 40.1). Often, it is associated with other conditions causing thrombi, but not infrequently, its cause remains unknown. CVT commonly presents with isolated headache but also must be kept on the differential for causes of cerebral ischemia, hemorrhage, and even coma. CVT image findings may be subtle but are important because overlooking them can have catastrophic consequences. Treatment recommendations for CVT had been controversial for many years, although anticoagulation remains the mainstay of treatment. Overall, the outcome for CVT is positive; if it is treated early, recurrence rates are low.
EPIDEMIOLOGY
CVT is an uncommon disorder affecting a variable patient population. CVT in adults is thought to affect about 5 people per 1 million every year. Most accounts estimate that CVT represents slightly less than 1% of all strokes. The International Study on CVT (ISCVT), the largest multicenter collaboration of consecutively enrolled symptomatic CVT patients older than 15 years with imaging confirmation, collected data on 624 patients from 24 countries and 89 centers and found the following epidemiologic data for CVT: median age was 37 years (age range 16 to 86 years), 74% of enrollees were female. These data is in keeping with the general belief that, although it can affect any age or sex, in the adult population, CVT is largely a disorder of young to middle-aged females.
The Canadian Pediatric Ischemic Stroke Registry (CPISR) is one of the largest pediatric CVT registries and involved 16 pediatric tertiary care centers in Canada collecting data on 160 consecutive cases of radiologically confirmed CVT in children 0 to 18 years old. These data demonstrated an incidence of pediatric CVT to be about 6.7 per 1 million people, slightly more common than adult CVT. Among the 160 children enrolled, 54% were younger than 1 year old (with 43% younger than 1 month of age) and 54% were male. This follows the general understanding that the pediatric CVT population largely involves very young children and the female preponderance seen in adult CVT is not present in pediatric CVT populations.
CVT has been attributed to numerous causes, yet even after extensive workup, almost 30% of CVT diagnoses remain idiopathic. ISCVT found that thrombophilia (34.1%) and oral contraception (54%, overall data corrected for females of childbearing age) accounted for a significant portion of the causes of CVT. Other important causes of CVT were puerperium (14%, overall data corrected for females of childbearing age) and pregnancy (6%, overall data corrected for females of childbearing age). Additionally, infection (especially of the ear, sinus, mouth, face, and neck) contributed to 12% of CVT cases in their data set, and malignancy (within and outside of the central nervous system [CNS], both solid tumor and hematologic) was found to have caused 7% of CVT in the ISCVT population. Regarding genetic causes, Marjot et al. performed a meta-analysis of 26 studies: This included 1,183 CVT patients, explored six genes, and demonstrated a statistically significant association between CVT and two genes: factor V Leiden (OR = 2.40; 95% CI, 1.75 to 3.30; P <.00001) and prothrombin gene mutation (OR = 5.48; 95% CI, 3.88 to 7.74; P <.00001). Finally, more than 44% of subjects were found to have more than one cause of CVT, an important fact to remember when exploring causes of CVT in hopes of preventing reoccurrence. Table 40.1 summarizes common causes of CVT.
In contrast to adult data, the most common cause of CVT in children is infection. In the CPISR data, acute infection was most commonly found in neonates (children younger than 1 month; 84%). Perinatal complications (51%) and dehydration (30%) were also common causes of CVT in the neonatal population. In older children (older than 1 month but younger than 18 years), chronic illness was the most common risk factor, especially connective tissue disorders (23%), hematologic disease (20%), and cancer (13%). Similar to the adult data, the CPISR data found prothrombotic states to be an important cause of CVT in neonates (20%) and children (54%).
CLINICAL FEATURES
The variable clinical presentation is one of the challenges of CVT. In adults, the disorder typically presents with symptoms attributed to increased intracranial pressure (ICP) associated with inability to drain the thrombosed vessel or focal neurologic disease ascribed to cerebral venous ischemia or hemorrhage.
Diffuse progressive headache over hours to days is the most common presentation in patients with CVT, although thunderclap and migrainous-type headache have also been described. Importantly, isolated headache without other neurologic findings or signs of elevated ICP occurred in 25% of confirmed CVT in the ISCVT cohort.
When CVT does cause an increase in ICP, patients commonly present with the following neurologic signs: papilledema, diplopia (most commonly due to sixth nerve palsy), headache which worsens with recumbency, nausea/vomiting, and encephalopathy. In addition to signs of increased ICP, focal neurologic deficits following cerebral ischemia or hemorrhage are also important clinical presentations in patients with CVT. The actual signs of the focal brain injury are attributed to the site of venous ischemia and are therefore variable but include focal weakness, sensory changes, visual field deficits, and aphasias. Further confounding this picture in CVT, the superior sagittal sinus, the most commonly involved cerebral venous structure in CVT, drains both cerebral hemispheres and therefore when thrombosed can cause bilateral deficits complicating neurologic localization. A small yet clinically important subset of CVT patients are those with deep CVT. CVT affecting the basal ganglia or thalamus is commonly bilateral and can lead to venous ischemia or hemorrhages. CVT affecting the deep parts of the brain tend to be more severe and quickly results in profound deficits including altered mental status and coma.
TABLE 40.1 Common Causes of Cerebral Sinus Thrombosis
Drugs
Oral contraceptives (especially in combination with tobacco and/or prothrombotic disease), hormone replacement therapy, asparaginase chemotherapy, tamoxifen, steroids, androgens
CNS tumors with invasion of the venous sinus, hematologic cancers, hypercoagulable state due to malignancy
Obstetric
Pregnancy and puerperium
Trauma (including iatrogenic)
Head injury, lumbar puncture, neurosurgical procedures
CNS, central nervous system.
Adapted from Frontera J, ed. Decision Making in Neurocritical Care. New York: Thieme; 2009.
The cavernous sinuses are a unique set of cerebral sinuses. They are deep bilateral structures at the base of the cerebrum that house the internal carotid artery, ophthalmic vein, branches of the sphenoid and superficial middle cerebral veins, as well as cranial nerves III, IV, V1, V2, and VI. Venous thrombosis affecting the cavernous sinuses are associated with palsies affecting these cranial nerves as well as pain, ptosis, chemosis, and proptosis. Increased intraocular pressure due to poor venous drainage can lead to loss of visual acuity. Most cavernous sinus thromboses are related to infection, typically due to Staphylococcus aureus, although Streptococcus pneumoniae, gram-negative rods, anaerobes, and occasionally fungal infections may be culprits. Spread of symptoms to the contralateral eye via the intracavernous sinuses may occur within 24 to 48 hours of the initial presentation and is pathognomonic for cavernous sinus thrombosis. Table 40.2 summarizes common syndromes associated with CVT.
TABLE 40.2 Common Cerebral Venous Thrombosis Syndromes
CVT Location
Symptoms
Superior sagittal sinus
Large vein, symptoms depend on location affected
Motor deficits (can be bilateral due to central location)
Psychiatric symptoms (when affecting the frontal lobes)
Seizures due to cortical location
Transverse sinus
Aphasias when they affect areas of speech
Cerebral cortical vein
Deficit varies depending on location of CVT Seizures due to cortical location
Deep venous system
Change in mental status
Coma
Bilateral deficits due to central location
Cavernous sinus
Palsies affecting cranial nerves III, IV, V1, V2, or VI
Orbital pain
CVT, cerebral venous thrombosis. Adapted from Frontera J, ed. Decision Making in Neurocritical Care. New York: Thieme; 2009.
Clinical presentation for CVT in children is similar to adults except in neonates where seizure is more common. In the CPISR database, 71% of neonates (children younger than 1 month old) with CVT had seizure attributed to CVT, in contrast to only 48% of non-neonate CPISR children and 44% of CVT patients older than 15 years.
Only gold members can continue reading. Log In or Register to continue