Chapter 100 CyberKnife Radiosurgery for Spinal Neoplasms
The successes of cranial stereotactic radiosurgery (SRS) inspired the development of spinal SRS.1–4 In little more than a decade, spinal SRS has revolutionized the treatment of spinal tumors and vascular malformations. The introduction of CyberKnife™ has allowed the delivery of very large doses of radiation to small lesions while sparing adjacent normal structures. CyberKnife™ outcomes are comparable or superior to those obtained with conventional radiotherapy, frame-based stereotactic systems, or conventional surgery.1–13 Since 1994, the CyberKnife™ has been used to treat over 10,000 spinal lesions at more than 200 sites worldwide.
Technology Overview
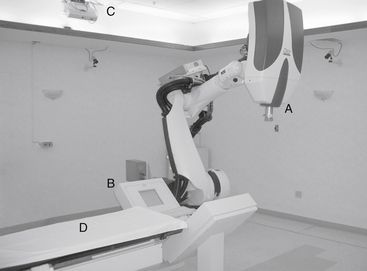
The CyberKnife system consists of a lightweight, 6-megavolt (MV) linear accelerator (LINAC) mounted on an industrial robot, a remotely repositionable treatment couch, orthogonally placed digital x-ray cameras, a treatment-delivery computer, and treatment planning stations (Fig. 100-1). During treatment, numerous images are obtained to optimally locate the target before the delivery of 100 to 150 individual treatment beams.14 The CyberKnife can deliver individual beams to any part of a tumor from nearly any angle and provides highly conformal dosing to complex three-dimensional (3D) targets.15
Treatment Details
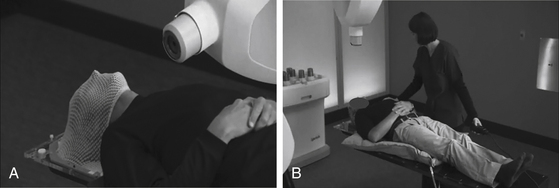
Spinal SRS is image guided and completely frameless. Individually molded masks or cradles are fashioned before the planning scans are completed. The patient rests in the mask or cradle during computed tomography (CT) scanning, magnetic resonance imaging (MRI), 3D angiography or positron emission tomography (PET) imaging, and again during treatment. The devices are comfortable, limit movement, and expedite positioning. At Stanford, we use an Aquaplast mask (WFR Corp., Wyckoff, NJ) for upper cervical lesions (Fig. 100-2A). Lower cervical, thoracic, lumbar, and sacral lesions are treated using an AlphaCradle (Smithers Medical Products, Akron, OH) (Fig. 100-2B). Most patients are treated supine but prone and lateral decubitus positioning is possible.
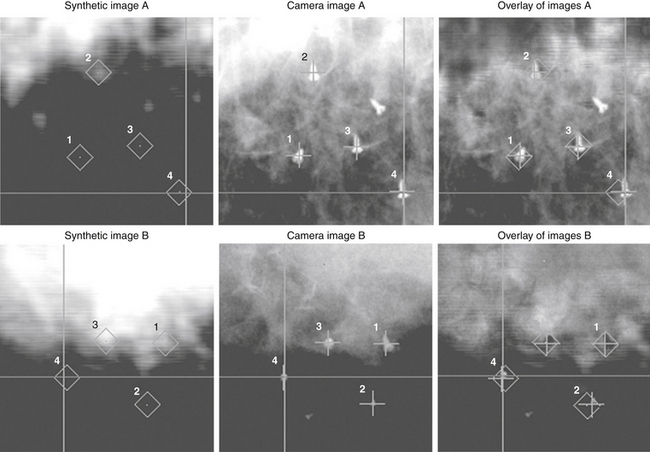
Bony landmarks are used to target spinal lesions and those in adjacent structures. Spinal fusion hardware does not interfere with treatment. The accuracy of CyberKnife approaches ±0.5 mm.7,16 For lesions not associated with bony landmarks, three or more gold seeds or titanium screws are implanted (Fig. 100-3).13,15
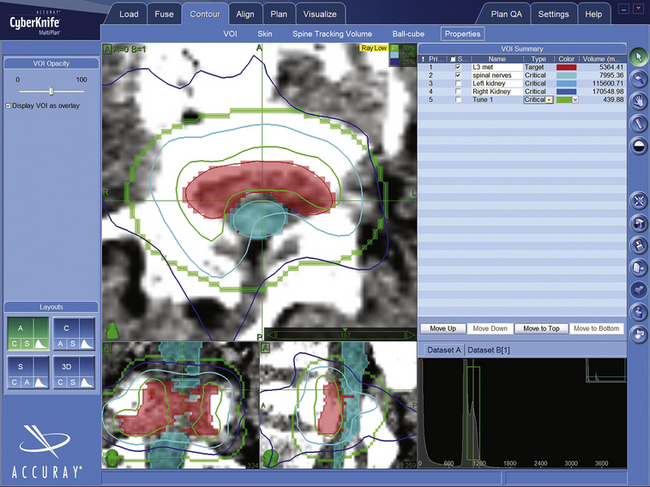
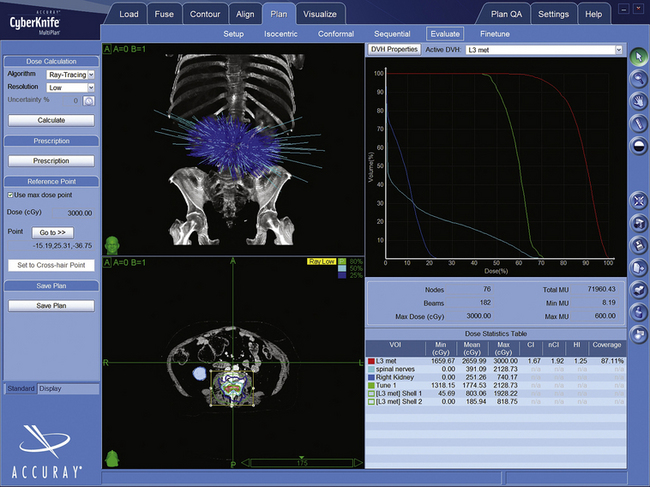
CyberKnife treatment plans use Accuray’s MultiPlan software. BrainLab, Varian, and Elekta systems employ similar programs. After uploading the CT and other images to the planning station, the surgeon and radiotherapist “contour” the target and radiation-sensitive structures by tracing their outlines (Fig. 100-4). The dose and number of sessions, as well as dose limits for adjacent structures, are prescribed by the physicians (Fig. 100-5). Physicists then use the planning system, the contour data, and the dose prescriptions to create a 3D representation of the lesion geometry and define sets of treatment beams. An ideal treatment includes evenly distributed beams that target the dose uniformly while limiting exposure to sensitive structures (Fig. 100-6). The neurosurgeon and/or physicist will iteratively perfect the plan by adding or removing constraints, or re-positioning individual beams. A multidisciplinary team reviews and accepts each treatment plan before delivery.
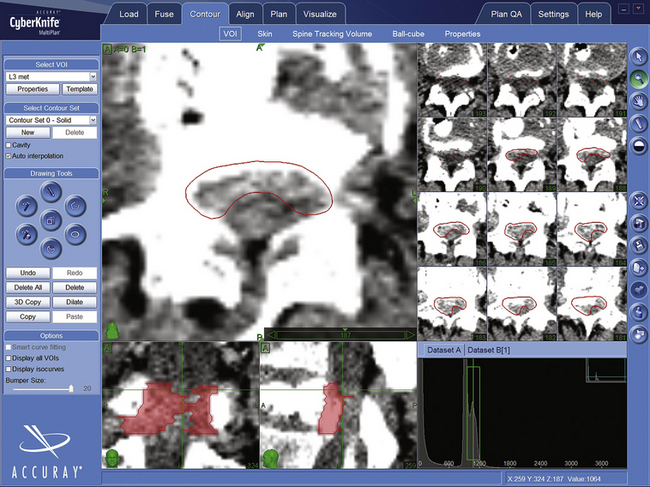
FIGURE 100-4 Contour of L3 metastasis in axial, saggital, and coronal projections. The epidural metastasis is in red.
Indications
It cannot be emphasized enough that the indications for spinal SRS continue to evolve quickly; spinal SRS is a new subdiscipline within neurosurgery and only now are standardized procedures for its application being developed. At our institution, we most frequently treat metastases, small benign tumors, postoperative residuals, lesions that recur following conventional surgery or radiation, vascular malformations, inoperable tumors, and lesions in those who decline surgery (Tables 100-1 and 100-2).3,7,13 Spinal lesions appropriate for CyberKnife™ radiosurgery should be reasonably well circumscribed, clearly visible on CT or MRI, and smaller than approximately 5 cm in diameter. We do not insist on obtaining a biopsy in advance of treatment if the diagnosis is clear from preradiosurgical imaging studies.
Table 100-1 Indications and Contraindications for Stereotactic Spinal Radiosurgery
| Indications | Contraindications |
|---|---|
| Progressive but minimal neurologic deficit Postresection or post-RT local irradiation (boost) Disease progression after surgery and/or irradiation Inoperable lesions or high-risk lesion locations Medical comorbidities that preclude surgery Lesions in patients who decline surgery | Spinal instability (adjunctive treatment only) Neurologic deficit caused by bony compression Severe neurologic deficit due to cord compression Adjacent cord previously radiated to maximum dose Very rare lesions not responsive to ionizing radiation |
Table 100-2 Treated/Treatable Lesions with CyberKnife Radiosurgery
| Tumors |
| Benign |
| Neurofibroma, schwannoma, meningioma, hemangioblastoma, chordoma, paraganglioma, ependymoma, epidermoid |
| Malignant/Metastatic |
| Breast, renal, non–small-cell lung, colon, gastric and prostate metastases; squamous cell (laryngeal, esophageal, and lung) tumors; osteosarcoma; carcinoid; multiple myeloma; clear cell carcinoma; adenoid cystic carcinoma; malignant nerve sheath tumor; endometrial carcinoma; malignant neuroendocrine tumor |
| Vascular Malformations |
| Arteriovenous malformation (types 2 and 3) |
Extradural Metastases
The spine is the most common site for bony metastases, accounting for nearly 40% of osseous tumor spread.17 Forty percent of cancer patients will develop at least 1 spinal metastasis.18 Historically, spinal metastases have been managed with chemotherapy, radiopharmaceuticals, surgery, and external beam irradiation.17,19 Conventional irradiation of spinal metastatic tumors is useful for palliation but its effectiveness is limited by spinal cord tolerance.20 Moreover, relapses are common,21–24 and retreatment with RT is generally impossible.18 SRS enables much larger biologically effective doses to be delivered by utilizing a more highly conformal plan that protects the cord. Multiple courses of spinal SRS can control multiple asynchronous metastases, and SRS may be used to sterilize a vertebral body before vertebroplasty25 or following a debulking procedure. The presence of spinal fusion hardware is not a contraindication.26 SRS is ideal for those with limited life expectancies or those who need other treatment. Most SRS treatments are completed in a single 1-hour session.
Treatment protocols in the published literature vary greatly and there is significant debate regarding the most appropriate treatment margins.27 For purely bony lesions, Amdur et al.27 recommend treating visible tumor plus a 1-cm margin in bone or a 2-mm volume outside the external cortex. For lesions within the canal, the margins are not extended beyond the visible tumor. Many groups irradiate the entire affected vertebral body including the pedicles. Chang et al.18 recommend treating the pedicles for possible tumor extension, pointing out that 18% of recurrences occurred in the pedicles. At Stanford we typically treat the tumor volume as seen on CT or MRI.17 There are no studies that show a clear benefit of one approach over the other, but those who treat smaller volumes argue that the cord dose is decreased and that recurrences can be retreated. Dose recommendations are variable with single-session prescriptions ranging from 8 to 24 Gy in the published literature.27 At Stanford we have used from 16 to 25 Gy in up to five fractions, but usually opt to treat in the fewest possible sessions as dictated by the length and dose of irradiated spinal cord.17
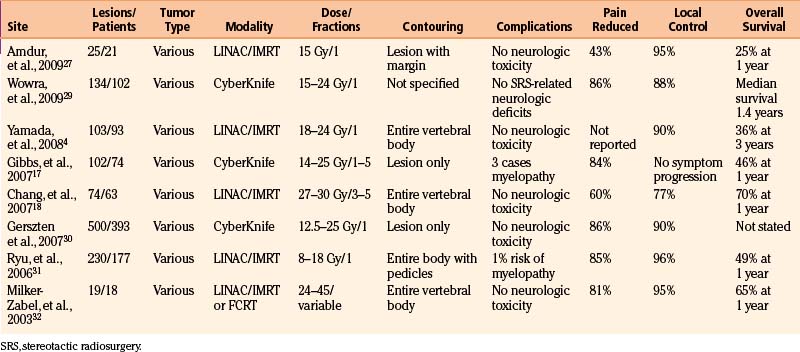
Overall the efficacy of radiosurgery for spinal metastases appears roughly comparable to that for brain metastases.2,3,17 Tumor growth is arrested by radiosurgery in up to 100% of cases and results are independent of histology (Table 100-3).4,28 Pain relief ranged from 43% to 96% and unlike standard RT, is generally apparent within days of SRS.27
< div class='tao-gold-member'>
Related posts:
 Cortical and Subcortical Brain Mapping
Cortical and Subcortical Brain Mapping
 Radiation Therapy and Radiosurgery in the Management of Craniopharyngiomas
Radiation Therapy and Radiosurgery in the Management of Craniopharyngiomas
 Surgical Management of Intracerebral Hemorrhage
Surgical Management of Intracerebral Hemorrhage
 Contemporary Dorsal Rhizotomy Surgery for the Treatment of Spasticity in Childhood
Contemporary Dorsal Rhizotomy Surgery for the Treatment of Spasticity in Childhood
 Role of Gamma Knife Radiosurgery in the Management of Arteriovenous Malformations
Role of Gamma Knife Radiosurgery in the Management of Arteriovenous Malformations
 Arachnoid, Suprasellar, and Rathke’s Cleft Cysts
Arachnoid, Suprasellar, and Rathke’s Cleft Cysts
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


