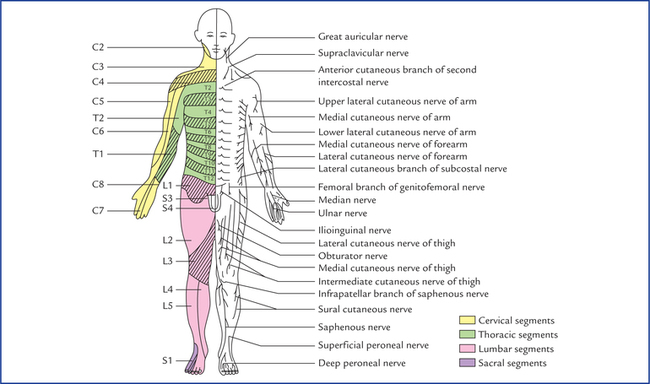
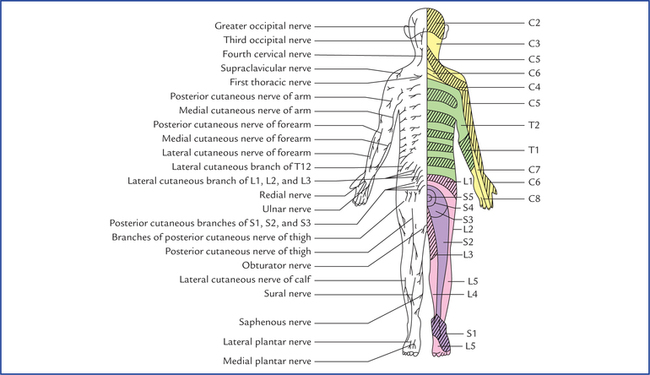
5 An accurate assessment of the degree and type of cutaneous sensory impairment and muscular activity play a key role in making the correct diagnosis of a neurological disease. The students, therefore, should have clear concept of segmental innervation of skin and muscles. In the trunk the arrangement of dermatomes is simple because the thoracic and upper lumbar spinal nerve supplying it are arranged segmentally. On the trunk the dermatome extends around the body from the posterior median line to the anterior median line. Figures 5.1 and 5.2 depict the dermatomal maps for the anterior and posterior surfaces of the body. Adjacent dermatomes overlap considerably (Fig. 5.3); therefore to produce a region of complete anaesthesia at least three contiguous nerves have to be severed. Further, it is important to note that the area of tactile loss is always larger than the area of loss of thermal and painful sensations. This is due to the fact that the degree of overlap of fibres carrying pain and temperature sensations is much more extensive than the overlap of fibres carrying tactile sensations. Fig. 5.1 Anterior aspect of the body showing the pattern of dermatomes on the left side, and distribution of cutaneous nerves on the right side. Fig. 5.2 Posterior aspect of the body showing pattern of dermatomes on the right side and distribution of cutaneous nerves on the left side. Fig. 5.3 (A) The rotation of the limbs during embryonic development. (B) The arrangement of dermatomes in the upper and lower limbs of the embryo. In early embryonic development, the upper and lower limbs appear as paired paddle-shaped limb buds. Each bud has preaxial and postaxial borders, with former being towards the head. Later in the development the ends become expanded and flattened to form hand and foot plates, in which the digits develop. The digits along the preaxial border are the thumb and big toe. The limbs then rotate. The upper limb rotates laterally so that its preaxial border and thumb come to lie on the lateral side. On the other hand, the lower limb rotates medially and its preaxial border and big toe come to lie on the medial side. It is now easier to understand why the dermatomes innervated by spinal nerves of brachial plexus are arranged consecutively down on the lateral side and up on the medial side of the upper limb, and dermatomes innervated by spinal nerves of lumbosacral plexus are arranged down the medial side and up the lateral side and back of the lower limb (Fig. 5.3 A, B). In the head and face region, each of the three divisions of the trigeminal nerve supply a precise area of skin and there is little or no overlap to the cutaneous area of the another division (Fig. 9.8). • Because of the development of the upper limbs the anterior primary rami of lower cervical and first thoracic spinal nerves have lost their cutaneous innervation of the trunk anteriorly, and at the level of the sternal angle, the fourth cervical der-matome is contiguous with the second thoracic dermatome (Fig. 5.1). • During the development of head and neck, due to upward migration of upper cervical dermatomes the back of the head is supplied by upper cervical spinal nerves, and at the interauricular line, the second cervical dermatome is continuous with the cutaneous area innervated by the trigeminal nerve (Figs 5.1 and 9.9). It is important to note the following facts carefully: • Most of the skeletal muscles are supplied by two or more spinal segments (the intrinsic muscles of the hand are exception as they are unisegmental). • Muscles sharing a common primary action are supplied by the same spinal segments and the opposing muscles by the lower segments in sequence with the former. For example, the flexors of the elbow joint are supplied by C5 and C6 spinal segments and the extensors by the C7 and C8 spinal segments. • There is correlation among the innervation of muscles, joints and the skin, i.e. the branches of those spinal nerves which supply the muscles moving a joint also supply the skin over the insertions of the same muscles and the interior of the joint.
Dermatomes and Muscular Activity
Segmental Innervation of Skin

Segmental Innervation of Muscles
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Neupsy Key
Fastest Neupsy Insight Engine






