Wave form of the V2 segment of the vertebral artery with progressive luminal narrowing of the subclavian artery [2]. Stepwise development of retrograde flow: decelerated upstroke (A), systolic deceleration (B), alternating flow (C) and reversed (D) flow.
Collateral systems
Preexisting communicating channels are employed as soon as pressure gradients occur. In the case of extracranial internal carotid artery (ICA) occlusions and high-grade stenosis, only those anastomoses are relevant which have the potential to bypass the obstruction along the reversed ophthalmic artery to the carotid siphon. In the case of common carotid artery (CCA) occlusion, normal ICA perfusion is occasionally maintained by retrograde blood flow in the external carotid artery (ECA) (Figure 11.2).
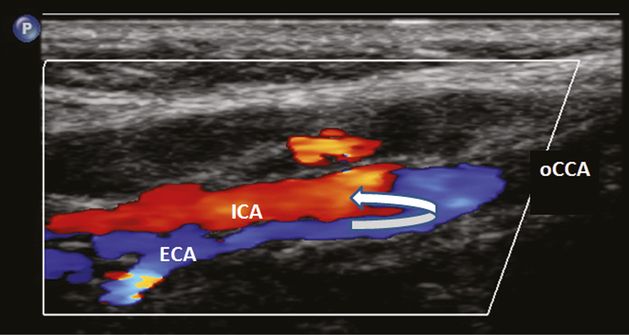
Occlusion of the common carotid artery (oCCA) with patent bifurcation. Internal carotid artery (ICA) is fed by reversed flow from the external carotid artery (ECA).
Ophthalmic artery anastomosis
With respect to the pressure gradient, the periophthalmic arteries are interposed between the ECA and ICA territory in a “watershed” situation. If a significant pressure drop occurs in the ICA, blood flow may be directed from the periorbital area to the siphon along the reversed ophthalmic artery (OA). The detection of retrograde blood flow in the OA has an important diagnostic implication because it represents a main criteria for the classification of high-grade ICA stenoses (see Chapter 5C).
Retrograde blood flow in the supraorbital artery (SA) can be reliably detected by means of a pencil probe continuously emitting 8 MHZ including the application of compression tests (Figure 11.3). Color duplex sonography may allow visualization and differentiation of complex collateral networks in the neck tissue which bypass segmental VA occlusions.
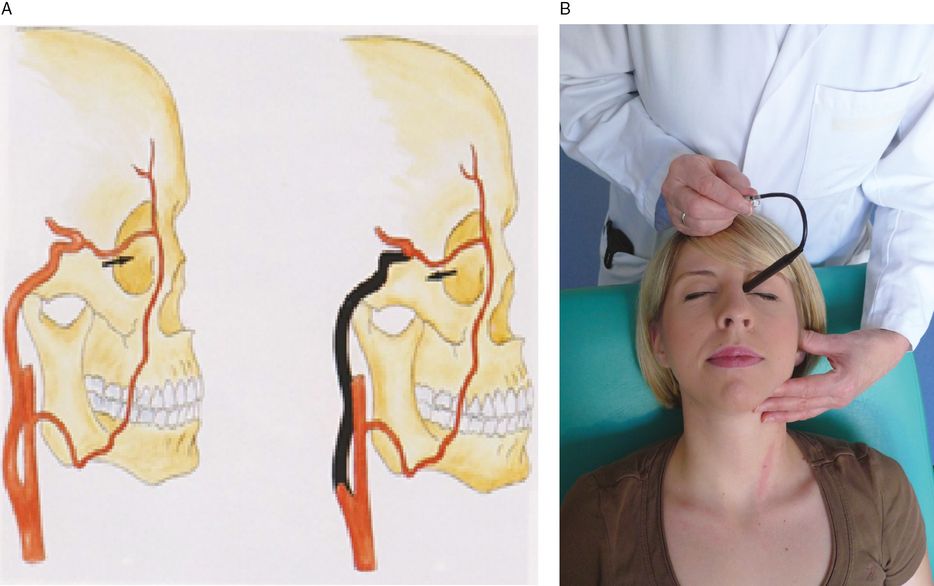
(A) The ophthalmic collateral [3]. Reversed flow in the supratrochlear artery in case of high-grade obstruction in the ICA proximal to the ophthalmic artery origin. The scheme shows the connection from the ECA via the facial artery to the ophthalmic artery. There are more anastomoses (i.e., superficial temporal artery) which are not shown in this picture. (B) Examination technique. Simultaneous compression of the superficial temporal artery and the facial artery. Ipsilateral compression may evoke flow reversal, zeroflow or increasing antegrade flow. The probe rests loosely at the medial canthus of the eye.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


