Intracerebral hemorrhage (ICH) is defined as the acute spontaneous bleeding into the brain parenchyma (Fig. 38.1). Primary ICH results from microscopic small artery degeneration in the brain, caused either by chronic, poorly controlled hypertension (80% of cases) or amyloid angiopathy (20% of cases). Secondary ICH refers to intraparenchymal bleeding from a diagnosable anatomic vascular lesion or cause of coagulopathy (Table 38.1).
EPIDEMIOLOGY
The overall incidence of ICH is estimated to be 12 to 15 cases per 100,000/yr. As the least treatable and most devastating form of stroke, ICH is a leading cause of mortality, morbidity, and disability in the United States and worldwide, accounting for 10% to 30% of all stroke hospital admissions. Many ICH patients require long-term health care, and only 20% of patients regain functional independence. About 40% to 80% of ICH patients die within the first 30 days, and half of all deaths occur within the first 48 hours.
RISK FACTORS
Hypertension and older age are the strongest predictors of incident ICH. Studies have shown that noncompliance with antihypertensive medications increases the risk of ICH, and control of blood pressure has been shown to reduce this risk. Chronic hypertension causes a small-vessel vasculopathy characterized by fragmentation, degeneration, and the eventual rupture of small penetrating vessels within the brain termed lipohyalinosis. Commonly affected structures include the basal ganglia and thalamus (50%), lobar regions (33%), and brain stem and cerebellum (17%). On pathologic examination, the pattern of small-vessel damage is characterized by (1) degeneration of medial smooth muscle cells; (2) small miliary aneurysms associated with thrombosis and microhemorrhages; (3) accumulation of nonfatty debris; and (4) hyalinization of the intima, preferentially at bifurcation points and distal portions of the vessel. It is unclear why some patients develop deep brain infarcts and others develop hemorrhages, but some have implicated the sudden rupture of microaneurysms, also known as Charcot-Bouchard microaneurysms, as the basis for ICH. Other nonmodifiable risk factors for ICH include male gender and African-American or Japanese race/ethnicity.
Low cholesterol levels have been implicated as a risk factor for primary ICH, although there is controversy regarding this association, as the results from case-control and cohort studies and prospective randomized trials of cholesterol reduction have yielded conflicting results. Heavy alcohol intake has been implicated as a risk factor for ICH in several studies. In theory, alcohol may affect platelet function and coagulation physiology and enhance vascular fragility.
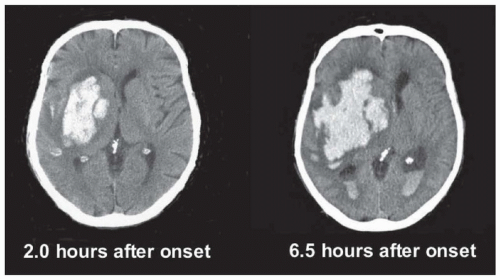
FIGURE 38.1 Basal ganglia ICH with hematoma followed by expansion and IVH.
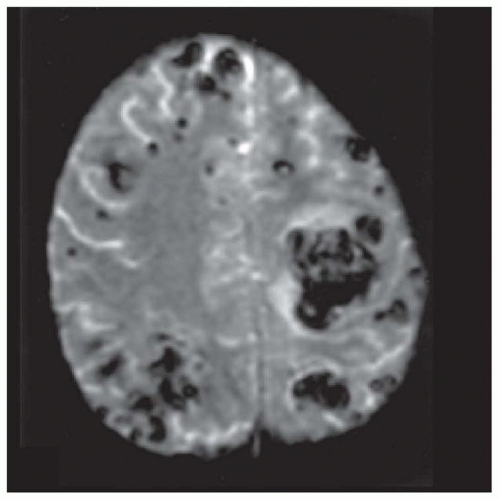
Cerebral amyloid angiopathy (CAA) is an important risk factor for ICH in the elderly (Fig. 38.2). CAA is characterized by the deposition of β-amyloid protein in small- to medium-sized blood vessels of the brain and leptomeninges, which may undergo fibrinoid necrosis. It can occur as a sporadic disorder, in association with Alzheimer disease, or with certain familial syndromes (apolipoprotein E2 and E4 allele). Brain tumors, sympathomimetic drugs, coagulopathies, cavernomas, and arteriovenous malformations also cause brain hemorrhages. Further differential diagnoses of underlying pathologies are summarized in Table 38.1. Although treatment with anticoagulants or fibrinolytic agents entails a higher risk of hemorrhage with increasing doses, the role of aspirin intake in this context is controversial. The detection of microbleeds in gradient echo magnetic resonance imaging (MRI) implies that aspirin is a risk factor for hemorrhage in patients on anticoagulant therapy; MRI evidence of microhemorrhages should prompt reconsideration of the indications for anticoagulation.
TABLE 38.1 Etiologic Factors for Intracerebral Hemorrhage
Risk Factors for Primary Intracerebral Hemorrhage
Demographic
Age
Black race/ethnicity
Vascular risk factors
Chronic hypertension (small-vessel disease)
Alcohol
Smoking
Low cholesterol
Vascular pathology
Amyloid angiopathy (including hereditary forms)
Risk Factors for Secondary Intracerebral Hemorrhage
Brain infarction
Hemorrhagic transformation of subacute ischemic lesion
Abrupt arterial rupture leads to rapid accumulation of blood within the brain parenchyma and increase in local tissue pressure followed by the abrupt onset of shearing forces and physical destruction. In addition to the relative mass effect, the hematoma itself induces three early pathophysiologic changes in the surrounding brain tissue: (1) neuronal and glial cell death due to apoptosis and inflammation, (2) vasogenic edema, and (3) breakdown of the blood-brain barrier (BBB).
Hematoma expansion is an important cause of early neurologic deterioration, and ICH volume is a powerful predictor of outcome after primary ICH. An expanding hematoma may result from persistent bleeding and/or rebleeding from a single arteriolar rupture. Some studies have reported evidence of ICH growth from bleeding into an ischemic penumbra zone surrounding the hematoma, but studies have not confirmed the existence of ischemia in the hypoperfused area in the periphery of the hematoma. Because ischemia does not explain the changes and degree of neurologic dysfunction that occurs after the hemorrhage, neurotoxic and inflammatory mechanisms have more recently been implicated in the pathogenesis of perihemorrhagic tissue damage.
Peri-ICH edema may be produced by local and systemic inflammatory mediators that enhance tissue damage either directly or indirectly by the activation of leukocytes, generation of prostaglandins and leukotrienes, and activation of the complement. Intracerebral blood is in part directly responsible for the formation of local edema after ICH.
CLINICAL MANIFESTATIONS
Because most spontaneous hemorrhages arise from tiny vessels, the accumulation of a hematoma takes time and explains the smooth onset of the clinical syndrome over minutes or hours. The progressive course, frequent vomiting, and headache are major points that help to differentiate hemorrhage from infarction.
The putamen is the site most frequently affected. When the expanding hematoma involves the adjacent internal capsule, there is a contralateral hemiparesis, usually with hemianesthesia and hemianopia and, in large hematomas, aphasia or impaired awareness of the disorder. However, small self-limiting hematomas close to the capsular region may occasionally mimic lacunar syndromes featuring pure motor or sensory deficits. When the hemorrhage arises in the thalamus, hemianesthesia precedes the hemiparesis. Once contralateral motor, sensory, and visual field signs are established, the main points that distinguish the two sites are (1) conjugate horizontal ocular deviation in putaminal hemorrhage and (2) impaired upward gaze in thalamic hemorrhage. Pontine hemorrhage usually plunges the patient into coma with quadriparesis and grossly disconjugate ocular motility disorders, although small hemorrhages may mimic syndromes of infarction. Primary spontaneous hemorrhages within the mesencephalon or the medulla remain objects of debate and are rare curiosities. When they occur, the anatomic involvement is usually secondary to hemorrhage originating in neighboring diencephalic, cerebellar, or pontine regions. In the cerebral lobes, there is an as-yet-unexplained predilection for hemorrhages to occur within the posterior two-thirds of the brain. When they affect one or more cerebral lobes, the syndrome is difficult to distinguish, clinically, from infarction because progressive evolution and vomiting are much less frequent in infarction; also, lobar white matter hematomas often result from arteriovenous malformations, amyloid angiopathy, tumors, or other causes that only uncommonly affect the basal ganglia, thalamus, and pons.
Cerebellar hemorrhage warrants separate description because the mode of onset differs from that of cerebral hemorrhage and because it often necessitates surgical evacuation. The syndrome usually begins abruptly with vomiting and severe ataxia (which usually prevents standing and walking); it is occasionally accompanied by dysarthria, adjacent cranial nerve (mostly sixth and seventh) affection, and paralysis of conjugate lateral gaze to one side, findings that may mislead clinicians into thinking the disease is primarily in the brain stem. However, a cerebellar origin is suggested by the lack of changes in the level of consciousness and lack of focal weakness or sensory loss.
Enlargement of the mass does not change the clinical picture until there is enough brain stem compression to precipitate coma, at which point it is too late for surgical evacuation of the hemorrhage to reverse the disorder. This small margin of time between an alert state and an irreversible coma makes it imperative to consider the diagnosis in all patients with this clinical syndrome and is a reason to have patients who present in the emergency room with vomiting of undetermined origin attempt to stand and walk.
DIAGNOSTIC STUDIES
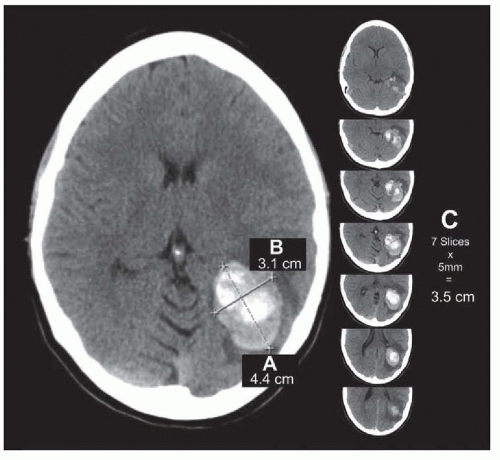
Nonenhanced computed tomography (CT) scan of the brain is the method of choice to evaluate the presence of ICH (see Fig. 38.1). CT scan evaluates the size and location of the hematoma, extension into the ventricular system, degree of surrounding edema, and anatomic disruption. Hematoma volume, a powerful predictor of 30-day mortality, can be easily calculated from CT scan images by use of the ABC ÷ 2 method, which involves multiplying the diameter of the hematoma in three dimensions and dividing by two (Fig. 38.3). CT angiography may reveal secondary ICH due to an aneurysm or arteriovenous malformation, or active contrast extravasation into the clot (“spot sign”), which implies an increased risk of early hematoma growth when identified soon after the onset of symptoms. MRI techniques such as gradient echo (GRE, T2*) are highly sensitive for the diagnosis of ICH as well (see Fig. 38.2). MRI in patients with atypical ICH patterns on CT may disclose a cause of secondary ICH (i.e., tumor, arteriovenous malformation, or hemorrhagic infarction up to 20% of cases). Conventional diagnostic cerebral angiography should be reserved for patients in whom secondary causes of ICH are suspected, such as aneurysms, arteriovenous malformations, cortical vein or dural sinus thrombosis, or vasculitis. Findings on CT scan or MRI that should prompt angiographic study include the presence of subarachnoid hemorrhage (SAH), intraventricular hemorrhage (IVH), underlying calcification, or lobar hemorrhage in nonhypertensive younger patients. Diagnostic catheter angiography should be strongly considered in all patients with primary IVH and younger nonhypertensive patients with lobar ICH.
FIGURE 38.3 ICH volume measurement. (A) Largest hemorrhage axial diameter. (B) Largest axial diameter perpendicular to A on same slice. (C) Vertical hemorrhage diameter (number of slices with hemorrhage multiplied by slice thickness). For this example, ABC/2 = (4.4 cm × 3.1 cm × 3.5 cm)/2 = 23.9 cm3. (From Beslow LA, Ichord RN, Kasner SE, et al. ABC/XYZ estimates intracerebral hemorrhage volume as a percent of total brain volume in children. Stroke. 2010;41:691-694, with permission.)
MEDICAL MANAGEMENT
Prehospital care of ICH follows similar guidelines as for other types of stroke, where the objective is to provide rapid access to medical facilities capable of dealing with stroke patients. In the emergency department, ICH patients should be triaged rapidly with CT scans to access stroke units or intensive care units (ICUs). Observation in an ICU or a similar setting is strongly recommended for at least the first 24 hours because the risk of neurologic deterioration is highest during this period and because the majority of patients with brain stem or cerebellar hemorrhage have depressed level of consciousness requiring ventilatory support. A protocolized checklist for care in the ICU is recommended to ensure standardization of best practices (Table 38.2).
TABLE 38.2 Medical Management Checklist for Acute Intracerebral Hemorrhage
Blood pressure
Maintain mean arterial pressure <140 mm Hg with continuous infusion labetalol (2-10 mg/min) or nicardipine (5-15 mg/h)
If stuporous or comatose, measure ICP and maintain CPP >70 mm Hg.
Reversal of anticoagulation
For elevated INR: vitamin K 10 mg IVP and 4F-PCC
INR 2 to <4: 25 U/kg; not to exceed 2,500 units
INR 4-6: 35 U/kg; not to exceed 3,500 units
INR >6: 50 U/kg; not to exceed 5,000 units
For heparin: protamine sulfate 10-50 mg slow IVP (1 mg reverses approximately 100 units of heparin)
For thrombocytopenia or platelet dysfunction: desmopressin 0.3 µg/kg IVP and/or transfuse 6 units of platelets
Expedited INR reversal for lifesaving neurosurgical intervention: recombinant activated factor VII 40-80 µg/kg (approximately 3.0-6.0 mg) IVP
Intracranial hypertension
Elevate head of bed to 30 degrees
Mannitol 1.0-1.5 g IV
Hyperventilate to PCO2 of 30 mm Hg
Fluids and nutrition
Normal (0.9%) saline at 1.0 mL/kg/h
Begin enteral feeding via nasoduodenal tube within 24 hours.
Seizure prophylaxis
For coma with intracranial hypertension or acute seizures: fosphenytoin (15-20 mg/kg) followed by 300 mg IV daily or levetiracetam 1,000 mg b.i.d. for 7 days
Physiologic homeostasis
Cooling blankets to maintain T ≤37.5°C
Insulin drip to maintain glucose 120-180 mg/dL
4F-PCC, four-factor prothrombin complex concentrate containing factors II, VII, IX, and X.
Only gold members can continue reading. Log In or Register to continue