 FIGURE 33.1 Compliance is the change in pressure per change in unit of volume (ΔP/ΔV). Once compensatory mechanisms are overwhelmed, compliance dramatically decreases, meaning that with a smaller increment in intracranial volume, a much more dramatic increase in pressure develops. |
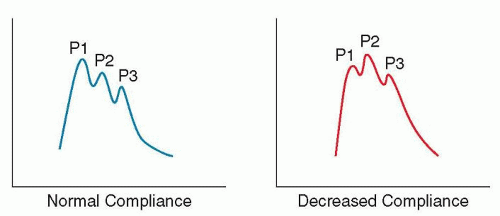 FIGURE 33.2 ICP waveform. P1, the percussive wave, comes from arterial transmission through the choroid plexus. P2, the tidal wave, reflects brain tissue elastance. As it rises, so does P2. When P2 exceeds P1, it has an excellent sensitivity to predict incoming increase in ICP. The third and final wave (P3) is secondary to aortic valve closure, a corollary of the arterial dicrotic notch. |
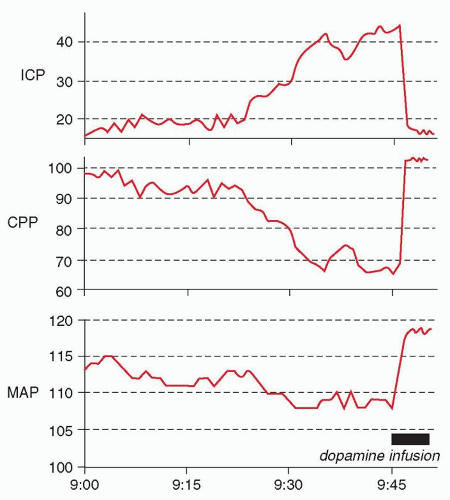 FIGURE 33.3 Lundberg A (plateau) wave, with characteristic “mirror” reduction in CPP. The plateau wave is terminated by an infusion of dopamine, which leads to an elevation in mean arterial pressure and reversal of the brain’s vasodilated state. ICP, intracranial pressure; CPP, cerebral perfusion pressure; MAP, mean arterial pressure. |
The patient is comatose (generally Glasgow Coma Scale [GCS] score ≤8).
Brain imaging indicates that the patient is at risk for elevated ICP due to the presence of significant intracranial mass effect.
Aggressive intensive care unit (ICU) care is warranted.
time, especially if associated with physiologic derangement, for example, during major surgery or a difficult to ventilate acute respiratory distress syndrome (ARDS) patient. Obstructive hydrocephalus is also a clear indication for EVD insertion. Recent guidelines from the International Multidisciplinary Consensus Conference on Multimodality issued recommendations for ICP monitoring in non-TBI patients (Table 33.2). Examples given in the consensus include massive ischemic stroke, meningitis, hypoxic-ischemic injury, and hepatic fulminant failure. Any pathology complicated by elevated ICP might benefit of such monitoring when clinical exam is not trustworthy, as it allows optimization of cerebral hemodynamics through CPP manipulation, aggressive ICP treatment, as well as detection of new catastrophic events.
TABLE 33.1 Indications for Intracranial Pressure Monitoring in Traumatic Brain Injury Patients | ||||||||
|---|---|---|---|---|---|---|---|---|
| ||||||||
TABLE 33.2 Indications for Intracranial Pressure Monitoring in Nontraumatic Brain Injury Patients | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


