Fig. 25.1
Standing Anteriorposterior and Lateral Scoliosis x-rays showing coronal and sagittal decompensation
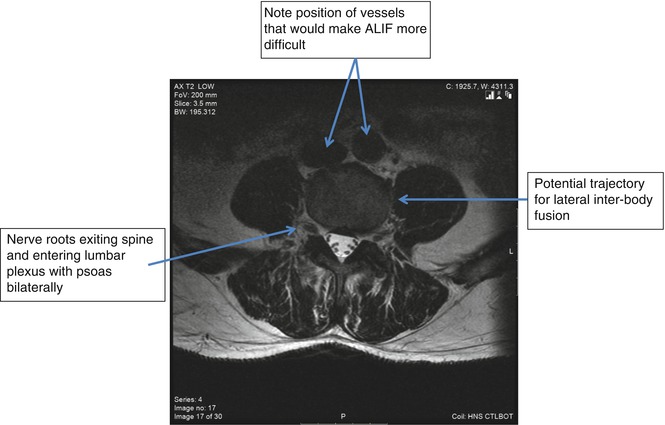
Fig. 25.2
Axial T2 Weighted slice through lumbar segment to illustrate position of the psoas
25.4 Concave Approach
Fortunately, approaching from the side that allows access to the L4–5 disc obliquity is usually approaching from the concavity of a lumbar scoliosis (Fig. 25.3). When approaching from the concavity, the surgeon is able to access multiple levels from one well-placed incision as depicted in Fig. 25.3. Once the decision to approach from the concavity has been made, the surgeon should consider addressing the cephalad or most caudal levels first rather than addressing the apical levels first which will correct the deformity and likely make access to the higher or lower levels more difficult because they will be further displaced upward under the ribs or lower into the pelvis, respectively. Angled instrumentation to access and prepare the disc spaces is now available from most manufacturers. These angled cob elevators, pituitary rongeurs, and curettes allow the surgeon to access, prepare, and release the disc while preserving the end plates.
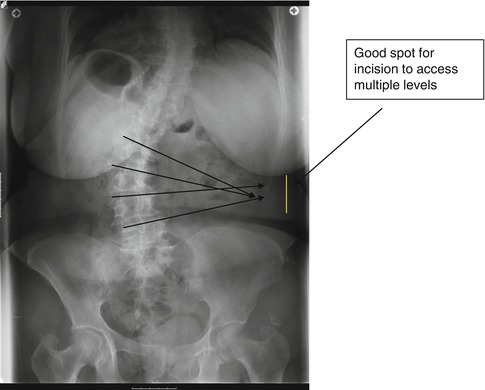
Fig. 25.3
Posterioranterior x-ray of the lumbar spine with lines drawn along endplates of each vertebrae demonstrating how to localize incision site
By addressing the curvature from the concavity, a significant amount of correction can be achieved in the coronal and sagittal plane deformities. Releasing the annulus of each disc and distracting the more collapsed side of the disc allow for the most significant correction. Approaching from the concavity also allows approach to the upper lumbar levels with less likelihood of entering the chest (Fig. 25.4). The operating table can be used to help correct the deformity when approaching from the concave side of the curve by flexing the break in the table (Fig. 25.5).
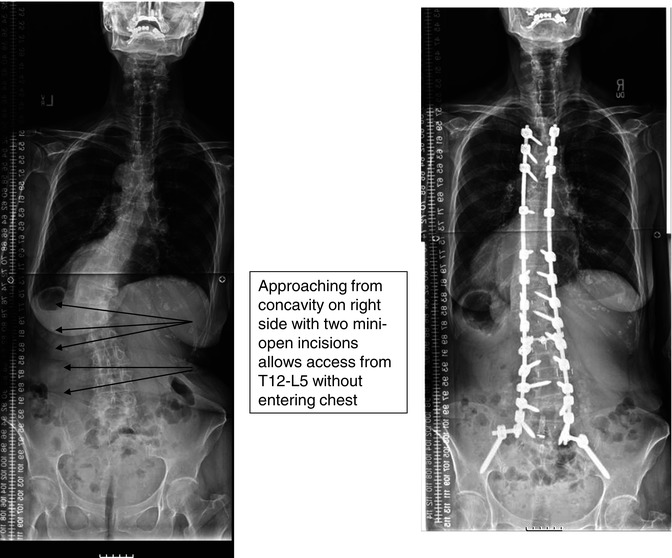
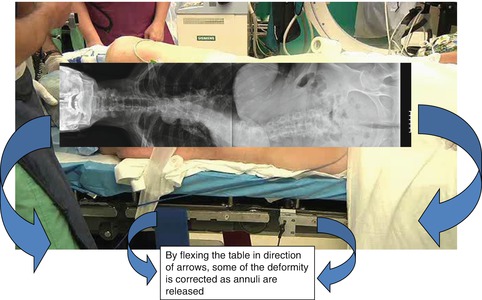
Fig. 25.4
Preoperative and postoperative posterioranterior standing scoliosis x-rays showing the correction achieved
Fig. 25.5
Clinical photograph of patient on operating table in left lateral decubitus postion with superimposed posterioranterior scoliosis x-ray demonstrating approach from concave side and how flexing the operating table would facilitate access to the spine
Care must be taken when approaching from the concave side to avoid excessive bony destruction. This is especially true in patients with large bridging osteophytes on the concavity of the curve. Using an osteotome to enter the disc space under fluoroscopic guidance in the anterior-posterior view from the concavity of the curve can help minimize bony destruction (Fig. 25.8). The position of the segmental vessels must also be considered with a concave-sided approach [14, 15]. The segmental arteries can be bunched together and may be prone to injury when removing concave osteophytes. Again, using the fluoroscopic guidance to be sure the trajectory of the osteotome remains in the plane of the disc will minimize the likelihood of injury to the segmental vessels.
In 30 cases of adult degenerative scoliosis, improvement of Oswestry Disability Index, Short Form-12, and Visual Analog scores for back pain improved by approach from the concave side at 130 levels without any increase in perioperative complications [16].
25.5 Convex Approach
In cases of a large lumbar scoliosis with extreme coronal decompensation, approach from the concavity may not be possible except to access the lower lumbar levels. Due to the extreme degree of coronal deformity and lumbar curvature in these cases, the upper lumbar disc spaces may actually be vertical and directed perpendicular to the floor when the patient stands, making approach from the concavity difficult if not impossible (Fig. 25.6). These upper discs may be brought into a more approachable position in patients with flexible curves, but in patients with rigid curves, the levels may not be approachable with a lateral technique without entering into the thoracic cavity usually from the convex side. In cases where approach to the lower levels can be facilitated by approach from either the concave or convex sides of the curve, partial correction can be achieved. This partial correction may make the upper lumbar levels more approachable through a second incision in a more orthogonal plane to the upper lumbar disc spaces usually from the concavity through a second incision to facilitate fusion if necessary (Fig. 25.7).
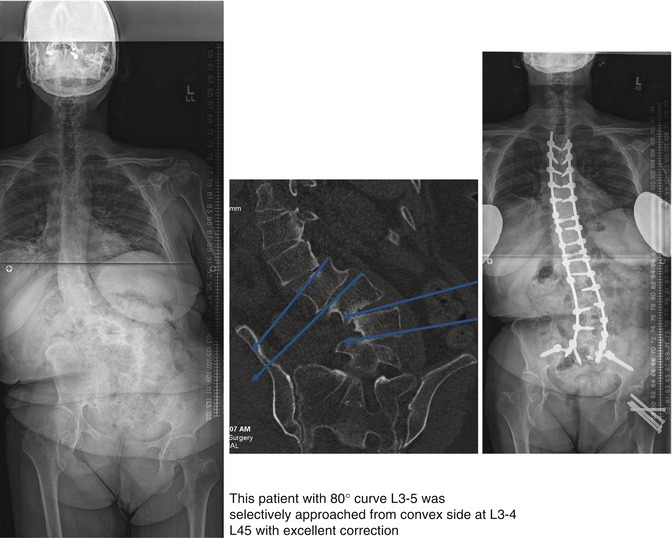

Fig. 25.6
Standing Anteriorposterior scoliosis x-ray and coronal CT scan image showing the difficulty that would be encountered with an attempt at access from the concave side in this patient. Anteriorposterior standing scoliosis x-ray showing final correction after approach from the convex side and posterior realignment
Fig. 25.7
Preoperative and postoperative coronal CT scan images showing lumbar spine
In cases where multiple incisions may be needed, especially when approaching a curve from the convexity, the lower lumbar incision is made where it will afford the best approach to the L4–5 level. It is usually possible to have access to L3–4 and L4–5 with this incision. Where the second, more cephalad incision will allow access to the L1–2 and L2–3 levels. Working in the disc space to release the annulus is somewhat easier coming from the convexity (Fig. 25.8).
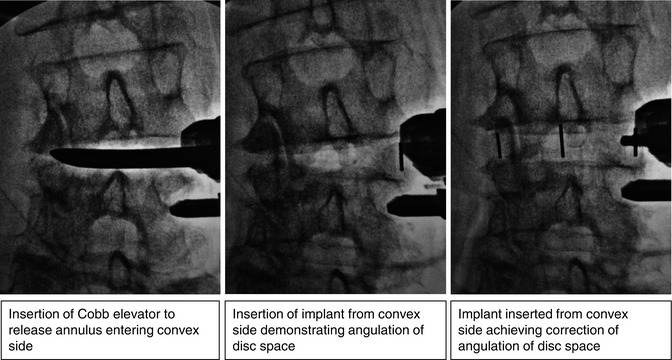
Fig. 25.8
 Costs of Minimally Invasive Spine Surgery
Costs of Minimally Invasive Spine Surgery
 Sagittal Balance
Sagittal Balance
 Lumbopelvic Parameters
Lumbopelvic Parameters
 Presacral Approach for Discectomy and Interbody Fusion in the Setting of Minimally Invasive Spine Surgery Deformity Correction
Presacral Approach for Discectomy and Interbody Fusion in the Setting of Minimally Invasive Spine Surgery Deformity Correction
 Minimally Invasive Thoracolumbar Facet Joint Fusion
Minimally Invasive Thoracolumbar Facet Joint Fusion
 Minimally Invasive Wiltse Approaches for Posterolateral Fusion
Minimally Invasive Wiltse Approaches for Posterolateral Fusion




Intraoperative floroscopic Anteriorposterior images showing release of the disc space and insertion of the interbody cage correcting the coronal segmental deformity and restoring disc space height
Related posts:
Costs of Minimally Invasive Spine Surgery
Sagittal Balance
Lumbopelvic Parameters
Presacral Approach for Discectomy and Interbody Fusion in the Setting of Minimally Invasive Spine Surgery Deformity Correction
Minimally Invasive Thoracolumbar Facet Joint Fusion
Minimally Invasive Wiltse Approaches for Posterolateral Fusion
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
