Fig. 31.1
(a and b) AP and lateral lumbosacral plain films of a 70-year-old female with degenerative scoliosis who underwent L4–L5 laminectomy elsewhere who presents with continued back pain and leg pain. Note the retrolisthesis at L3–L4, the spondylolisthesis at L4–L5, and the degenerated disc at L5–S1
31.1.1 Surgical Anatomy
Between the visceral and parietal fascia, in front of the sacrum, is an area known as the presacral space. The sacrum itself is separated from the rectum by a layer known as the mesorectum. In this layer, adipose tissue, lymphatics, and blood vessels are found. There are blood vessels in this space also such as the middle sacral artery [3]. Yuan et al. noted in a cadaveric study that there may be a safe zone along the anterior sacrum to perform a percutaneous approach [6]. They noted a distance along the anterior sacral margin to the rectum at the S3–S4 level as being approximately 1.2 cm on MRI and 1.3 cm on CT. They also noted a safe zone in terms of the distance between the right and left internal iliac vessels at S1–S2 of 6.9 cm on MRI and 6.0 cm on CT. They noted that the sacrum and its overlying parietal fascia provided a safe posterior border in which to potentially insert a blunt trocar to avoid structures anterior to the presacral space.
This corridor was actually first described by Cragg et al., where this corridor was used successfully for biopsy [1]. Eventually this was developed into a minimally invasive technique where discectomy and fusion could be performed [2]. Additionally, experience exists in the treatment of high-grade spondylolisthesis with transvertebral strut grafting, and this also influenced the design of this approach [7–9].
31.1.2 Device
To date, there is only one device available on the market for this approach. This is the AxiaLIF implant (Baxano Surgical, Raleigh, North Carolina). While initially the device was a single screw that was drilled into a channel through the sacrum, disc space, and L5 vertebral body over a guidewire, recent redesign has the device actually having four components. This allows selective internal distraction if necessary, by having a distraction rod internally rotate within the device with an S1 anchor and pushing on the shoulder with an L5 anchor to create distraction. Akesen et al. demonstrated rigid fixation for a single-level AxiaLIF supplemented with posterior instrumentation [10]. Similarly, Erkan et al. have shown rigid construct in presence of posterior fixation with a two-level AxiaLIF [11]. Most recently, Fleischer et al. compared S1 screw strain among four different constructs [12]. These included pedicle screws alone from L2 to S1, pedicle screws with anterior interbody fixation, pedicle screws with axial fixation, and pedicle screws with iliac screws. They showed that with pedicle screws alone, S1 screw strain was greatest. This was decreased by 38 % after anterior interbody augmentation, decreased by 75 % with axial fixation, and decreased by 78 % with pedicle screw and iliac screw fixation. This study demonstrated biomechanically that iliac screw fixation and AxiaLIF are quite similar in terms of the biomechanics with regard to protection of the S1 screw. Based on this biomechanical study, Boachie-Adjei et al. recommend using unilateral iliac screw for supplementation in spinal deformity correction when fusing to the sacrum and bilateral iliac screws for patients with osteoporosis [13]. However, they do not use any iliac screws for patients with normal bone mineral density where AxiaLIF is used in the setting of deformity correction. Our experience has been similar, where we also have not used iliac fixation for non-revision cases, where bone mineral density is within normal limits [14, 15].
31.2 Indications for the Presacral Approach for Discectomy and Fusion
Indications for using this approach include grade 1 degenerative spondylolisthesis, degenerative disc disease where fusion would be a consideration, interbody fusion in the setting of pseudarthrosis of a previous posterolateral fusion at L5–S1 or L4–L5 and L5–S1, and anterior column support in the setting of spinal deformity surgery. The approach to L4–L5 is also useful when the L4–L5 disc space is low and cannot be easily accessed via a transpsoas approach especially in deformity correction.
The presacral approach, however, has several important contraindications, including previous surgery in this region, history of prior colostomies, or pathology in the region of the rectum such as fistulas and also high-grade spondylolisthesis [3]. Any aberrant blood vessels in the region preclude this approach. Thus, a preoperative pelvic MRI is mandatory to exclude any aberrant midline vasculature at S1–S2 (Fig. 31.2). Additionally, adhesions are excluded. Especially if the patient has a history of inflammatory bowel disease, pelvic CT with a rectal contrast should also be considered to rule out any adhesions or aberrant rectal/sacral anatomy that would necessitate a different approach [16].
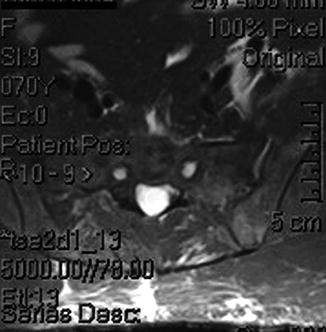
Fig. 31.2
Axial T2 MRI of the pelvis demonstrating normal midline at approximately the level of the S1–S2 segment: no midline flow voids are seen
31.2.1 AxiaLIF in the Setting of Deformity
Providing the decision is made as above, to fuse to the sacrum in the setting of deformity correction and a long fusion, we have suggested and agree with Boachie-Adjei et al. with regard to the AxiaLIF being a possible alternative to the use of iliac screws in cases of normal bone marrow density [13–15]. We confirm on 36-in. films the trajectory is appropriate. Additionally, preoperative sacral MRI is ordered to rule out aberrant pelvic vessels. If the history suggests any potential adhesions, our bias is not to do this procedure. All patients undergoing this procedure also undergo supplemental facet fusion. We use 2.1 mg of rhBMP-2 per disc space fused with this technique [17]. Additionally, in terms of the L5–S1 facets, we use approximately 1 mg of rhBMP-2 per facet-pars complex. Typically in our protocol for minimally invasive deformity correction, we will use a combination of three techniques [17–19]. These include the transpsoas discectomy and interbody fusion, the AxiaLIF if fusion extends to the sacrum, and multilevel percutaneous screws and rod placement. Typically, the AxiaLIF technique is performed prior to inserting pedicle screws unless there is preexisting lumbosacral junction obliquity. If there is obliquity present, we will typically correct it with screws prior to the transsacral fusion [18]. Additionally, we stress the importance of using tricortical pedicle screws as per Lehman et al [20]. We maximize the strength of our sacral fixation using a combination of this technique in addition to the AxiaLIF. In cases of revision surgery, or in the case of osteopenia, we have also used the S2 alar iliac technique to place collinear minimally invasive screws and avoid the need for extensive lateral dissection for iliac bolt placement [21, 22].
31.2.1.1 Procedure
The patient is positioned prone on a Jackson table. Extra padding is used to elevate the buttocks and legs. The legs are parted slightly to allow for the surgeon’s hand to follow the correct trajectory to enter for the AxiaLIF technique. Great care is taken not to place the buttocks strap, which would limit the operator’s excursion when performing this technique. The rectal area is prepped and isolated from the field (Fig. 31.3). Though others have recommended a bowel prep beforehand, we have not found this to be necessary [13, 23].

Fig. 31.3
Positioning for the AxiaLIF procedure. The patient is positioned prone on a Jackson table. The rectal area has been prepped and isolated from the field. Note that there is no thigh strap present that would limit excursion of the surgeon’s hand
For the actual technique, a 1-in. incision is planned over the midline by the sacrococcygeal junction. The skin is incised. A blunt probe is then introduced along the paracoccygeal notch, and in a controlled manner the fascia is pierced and presacral space entered. The hand is immediately dropped down between the legs to keep the tip of the blunt probe against the ventral surface of the sacrum. Strict biplanar fluoroscopy is then used. The probe is advanced along the ventral surface of the sacrum. Great care is taken not to deviate laterally into the ventral sacral foramina. The blunt probe is rested on the S1–S2 junction to allow for appropriate trajectory across the disc space. A sharp guidewire is introduced into the probe through the sacrum and advanced into the bone with a slap hammer. Using Seldinger technique principles, serial dilators are placed into the sacrum. Eventually, a 10-mm dilator (assembled with a dilator sheath) is slid over the other dilators and anchored into the sacrum using a cannulated slap hammer. Subsequently, the dilators and guide pin are removed while the 10-mm dilator sheath is left in place. A 9-mm cannulated drill is then placed over the guidewire and drilled to the sacrum up to the level of the L5–S1 disc space. Subsequently, that drill is removed, twisting in a clockwise manner in order to save bone as local bone autograft.
A radical discectomy then ensues. This entails using a series of nitinol rasps, radial cutters, and brush devices to remove disc material (Fig. 31.4). A thorough discectomy is performed. Subsequently, the disc space is irrigated out and grafted with local bone, demineralized bone matrix, and 2.1 mg of rhBMP-2 ACS using the manufacturer-supplied funnels [17].





