Fig. 34.1
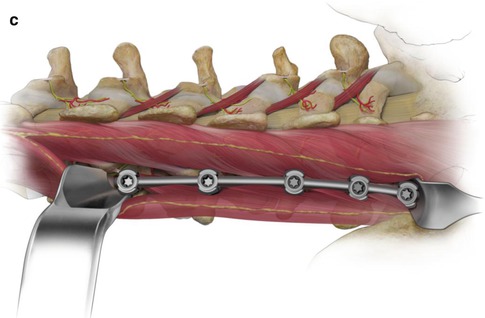
(a) The intermuscular plane is opened from L2 through sacrum. The common tendon of multifidus is seen inserting to the superior articular process at each segment. The longissimus fascicle arising from each accessory process is seen projecting towards a common tendon of insertion to the medial superior iliac spine. A bit of fat typically defines the dorsum of the intermuscular plane, with the entry adjacent to the spinous process at L1 and just medial to the iliac crest at the sacrum. The inset shows anatomy important to consider during screw placement and fusion. It is generally possible to place a screw just caudal and lateral to the medial branch of the nerve by being aware of the anatomy. (b) A right angle retractor may be used to engage the lateral articular process and retract the longissimus arising from the cephalad segment. The entry point for screw placement is seen on L2 just inferior to and lateral to the mammilloaccessory notch and nerve and at the upper margin of the tendon arising on the accessory process. Tap placement is seen at L3, with screw placement L4 to sacrum. The erector spinae aponeurosis is opened and retracted as necessary. (c) Screws are placed L2 through sacrum. The tendon and proximal longissimus lie between screw heads and may at times require a bit of division of the most dorsal portion of the tendon extending from the accessory process onto the mammilloaccessory ligament, to allow the rod to seat fully without unduly stretching the muscle and tendon. The assembled construct lies lateral to the multifidus complex with minimal impingement against back muscles
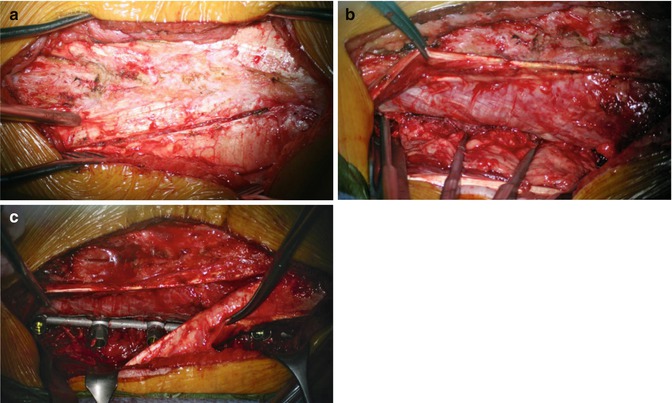
Fig. 34.2
(a) A midline skin incision has been made, with the dorsolumbar fascia reflected from L1 to the sacrum. The tendons of the ESA are seen projecting caudally to insertions on the dorsum of the spinous processes. The opening of the ESA is seen between tendons inserting to L4 and L5. (b) The upper medial ESA is reflected medially. The intermuscular plane is seen with the upper opening occurring near spinous process, adjacent to the spinous process. The tendons of the multifidus are seen forming on the lateral aspect of the multifidus to insert to the superior articular process (SAP). The retractor is seen engaged against the L1 SAP. Taps are in place in the pedicles L1 through L4. A bit of fat is appreciated in the deep plane between fascicles of longissimus. (c) The final construct is in place. Screws are seen in L1 through L3. The L4 screw underlies intervening ESA. The L5 and S1 screws are seen through a second opening in the ESA
A retractor engaging the lateral articular process retracts the longissimus traversing the transverse process and exposes bone for direct placement of a pedicle screw, with limited retraction of the longissimus. A screw entry point at the cephalad margin of the accessory process and 2–3 mm lateral to the lateral aspect of the mammillary process generally provides pedicle screw placement that respects the facet joint and mammilloaccessory notch.
Realizing that the spirit of MISS involves approaches preserving the anatomy rather than being defined by a skin incision, the illustrations reflect an anatomic approach opening intermuscular planes. This approach works for one or multiple segments and becomes easier with a multisegmental approach. While it is illustrated with a retractor engaging the articular process with limited retraction of the longissimus traversing from above, an awareness of the anatomy facilitates placement of a variety of retractors while taking advantage of an intermuscular construct placement. While the Wiltse approach has been used historically with decortication over the transverse process and articular complex, preservation of the back muscles is relatively straightforward. In a MISS situation, it may be appropriate to just decorticate inside the joint or extend the bony exposure along the lateral mass avoiding unnecessary neurovascular disruption.
It is my experience and impression that screw placement may respect the medial branch of the dorsal ramus most of the time. While it is difficult to visualize the nerve intraoperatively, an understanding of its course allows an entry generally sparing the mammilloaccessory notch and medial branch. There are certainly cases where maintaining an appropriate trajectory through the pedicle puts the nerve at risk, particularly in the upper lumbar spine, where divergence of the pedicles and articular complex necessitates encroaching to the region of the mammilloaccessory notch to avoid lateral compromise of the pedicle. With direct visualization and screw placement, it is appropriate to minimize Bovie use to preserve the nerve. Use of a cannulated screw with needle and wire to assist placement may also minimize risk to the nerve.
The erector spinae aponeurosis (ESA) is the tendon complex of the thoracic fascicles of longissimus and iliocostalis. This overlies the local back muscles with a medial trajectory to insertions on the dorsum of the spinous processes and across the distal sacrum and ilium. These tendons cross the intermuscular plane obliquely. Dividing the fibers over the underlying intermuscular plane generally allows easy exposure of three or four segments. A second parallel opening generally allows exposure of the entire lumbar spine with minimal difficulty encountered working under the preserved intervening tendons.
The dorsolumbar fascia is the aponeurosis of the latissimus dorsi. Reflecting this from adjacent to the spinous process provides a generous exposure for opening between the tendons of the ESA. A mediolateral opening along its fibers opens up the plane over the ESA and provides easy exposure for one or two segments. Exposing the entire lumbar intermuscular plane generally requires three or more openings in the dorsolumbar fascia if one wishes to avoid reflecting and reclosing this layer.
The skin incision is less critical in minimizing morbidity to lumbar muscles. At L3 and above mobilizing a midline incision for intermuscular approach is generally straightforward. When the dorsolumbar fascia is mobilized along the spinous process, retraction occurs over the ESA, avoiding a potential space for fluid collection or seroma superficial to the fascia. At L5–S1 and to a lesser extent at L4–5 mobilizing a short midline incision is more difficult because of the relatively lateral entry to the intermuscular plane, and short paramedian incisions are simpler for a short-segment construct.
34.3 Facet Fusion
The multifidus has a common tendon of insertion to each superior articular process. Figure 34.3 illustrates approach at the dorsal margin of the common tendon over the mammillary process that allows retraction of muscle traversing the lamina and facet capsule to caudal insertions. Opening the capsule of the joint allows decortication of the articular surfaces, with direct graft placement. This provides a robust facet fusion with no compromise of segmental muscle integrity. Extending decortication from the articular process to the lateral pars and base of the pedicle above, or to the laminar surface below, increases fusion, area with limited muscle disruption. For many years I have used a facet fusion only, when the articular processes have not been compromised and interbody grafting has been deemed unnecessary.
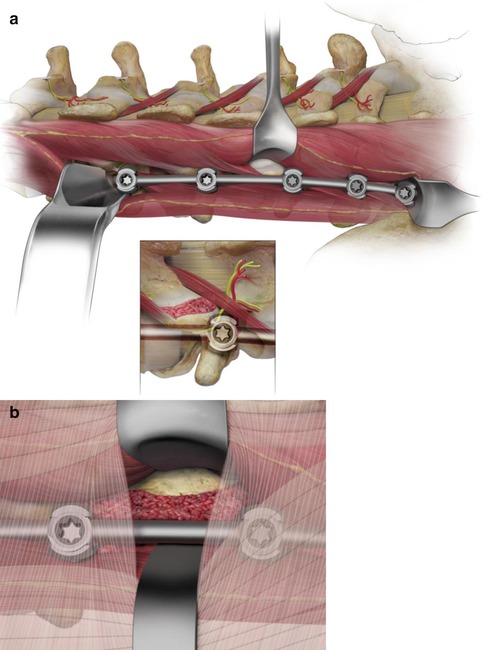
Fig. 34.3
(a) Approach at the caudal margin of the common tendon inserting to the SAP allows retraction of multifidus complex traversing to caudal levels. The retractor exposes the capsule of the facet joint and the lateral margin of the lamina and inferior articular process. The capsule of the facet joint is opened. This allows decorticating the facet joint with preservation of the integrity of the articular processes. The trajectory from the intermuscular plane allows optimal preparation of the joint for grafting. Bone graft is packed into the prepared joint before releasing the overlying muscle. (b) Disconnection of adjacent tendons on the SAP and accessory and transverse processes allows extending the graft for a more conventional lateral fusion in the situation where it is felt that sacrificing muscle is warranted for a more generous bony fusion. This view demonstrates both the ESA tendons separated to provide access to the joint and a mediolateral opening through the dorsolumbar fascia, preserving significant integrity to this layer with a segmented approach
Retraction is generally straightforward and I continue to use a variety of retractors to maintain visualization in the intermuscular plane. A malleable brain retractor may be bent slightly to engage the rod and folded at the skin to open the plane. An appropriate handheld retractor such a Langenbeck may then be used to retract muscle over the facet capsule for appropriate decortication and fusion in the joint.
While a facet fusion is adequately robust much of the time (Fig. 34.4), it is straightforward to extend through the inferior articular process to a transforaminal fusion. This may be done from the same opening used for the joint, or approach through the multifidus or down the lateral margin of the spinous process may provide a more medial, segmental approach while still preserving the muscles over the articular process.
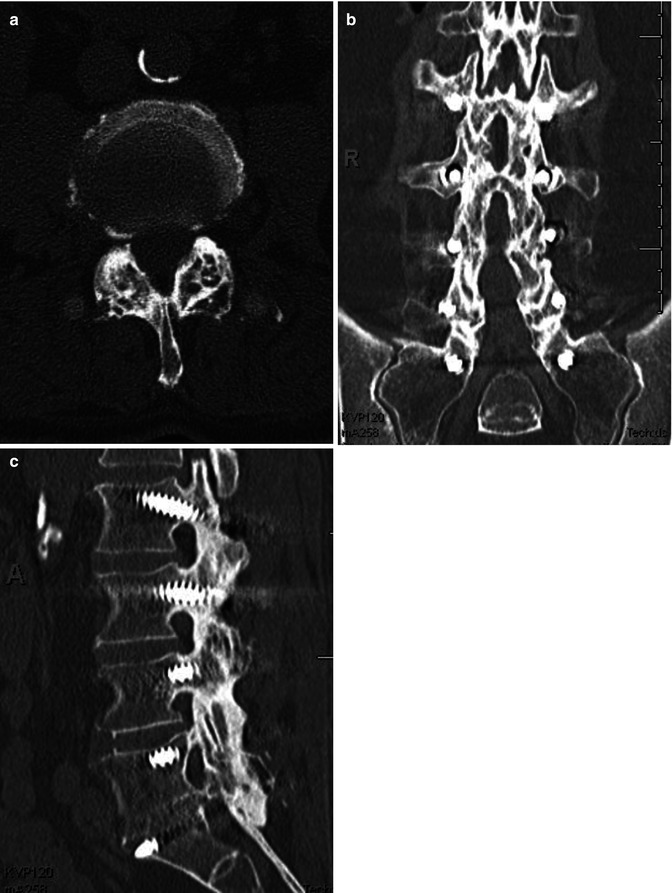
Fig. 34.4
(a) Axial section through a facet fusion. Peek rods are seen in cross section adjacent to the dorsal joint, in the intermuscular plane between multifidus and longissimus. (b) Dorsal view of reconstruction, demonstrating facet fusion along the articular complexes. (c) Lateral reconstruction demonstrating the robust fusion along the articular complex, with an interbody fusion at L5–S1
34.4 Medialized Segmental Approach to Fixation
A medial approach constrained by the muscle insertions to the superior articular process provides a complementary and equally anatomic approach to fixation and fusion. It is a segmental approach, rather than exposing the length of the lumbar spine, when the multifidus origins are preserved. In many cases, correction of deformity dictates osteotomies removing portions of spinous process or inferior articular process. Intervention is variably muscle sparing, however, and midline muscle disconnection optimizes exposure. In this situation the neurovascular integrity of the muscle is still preserved, and fixation across multiple segments is facilitated without exposure extending lateral to the superior articular process.
Related posts:
 Classification Schema for Scoliosis
The Importance of the Fractional Curve
Presacral Approach for Discectomy and Interbody Fusion in the Setting of Minimally Invasive Spine Surgery Deformity Correction
MIS in Adolescent Deformity
Minimally Invasive Thoracolumbar Facet Joint Fusion
Minimally Invasive Cement-Augmented Pedicle Screw Fixation
Classification Schema for Scoliosis
The Importance of the Fractional Curve
Presacral Approach for Discectomy and Interbody Fusion in the Setting of Minimally Invasive Spine Surgery Deformity Correction
MIS in Adolescent Deformity
Minimally Invasive Thoracolumbar Facet Joint Fusion
Minimally Invasive Cement-Augmented Pedicle Screw Fixation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


