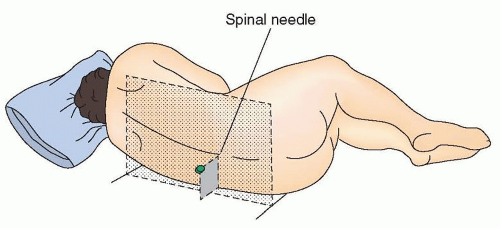
 FIGURE 31.1 Proper positioning for lumbar puncture. Position the patient’s back at the edge of the bed with the head flexed and the legs curled up in the fetal position. Place a pillow under the head. Hips are parallel to each other and perpendicular to the bed. The spinal needle should be parallel to the bed. (Adapted from Marshall R, Mayer S. On Call Neurology. 3rd ed. Philadelphia: Saunders; 2007.) |
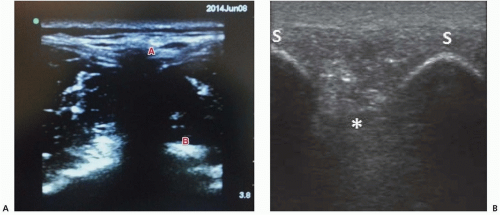 FIGURE 31.2 Ultrasound-guided LP. A: Transverse view. The anechoic shadow below A represents the spinous process—the midline; B localizes the transverse process. B: Longitudinal view. The interspace (asterisk) is located between the two crescentic-shaped, hyperechoic spinous processes (S). |
mononuclear cells. The cornerstone of etiologic diagnosis is the detection of viral nucleic acid sequences in the CSF via polymerase chain reaction (PCR). In cases of suspected viral meningoencephalitis, CSF PCRs for the enteroviruses along with the herpesviruses (herpes simplex virus 1 and 2, cytomegalovirus, varicella-zoster virus, Epstein-Barr virus (EBV), and in immunocompromised patients, human herpesvirus-6) should be sent, along with serologic testing for HIV. Serologic testing for several additional viruses can be considered (West Nile virus, St. Louis encephalitis virus, Eastern equine encephalitis virus, Venezuelan equine encephalitis virus, and La Crosse virus).
TABLE 31.1 Common Cerebrospinal Fluid Tests | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


