Anatomical Resection
Description
Surgical approach
Modifiers
Grade 1
Partial Facet Joint
Resection of the inferior facet and joint capsule at a given spinal level
A/P (anterior soft tissue release combined with posterior resection)
P (posterior approach only)
Grade 2
Complete Facet Joint
Both superior and inferior facets at a given spinal segment are resected with complete ligamentum flavum removal; other posterior elements of the vertebra including the lamina, and the spinous processes may also resected
A/P (anterior soft tissue release combined with posterior resection)
P (posterior approach only)
Grade 3
Pedicle/Partial Body
Partial wedge resection of a segment of the posterior vertebral body and a portion of the posterior vertebral elements with pedicles
A (anterior release)
P (posterior approach only)
A/P (both)
Grade 4
Pedicle/Partial Body/Disc
Wider wedge resection through the vertebral body; includes a substantial portion of the posterior vertebral body, posterior elements with pedicles and includes rejection of at least a portion of one end plate with the adjacent intervertebral disc
A (anterior release)
P (posterior approach only)
A/P (both)
Grade 5
Complete Vertebra and Disc
Complete removal of a vertebra and both adjacent discs (rib resection in the thoracic region)
A (anterior release)
P (posterior approach only)
A/P (both)
Grade 6
Multiple Vertebrae and Disc
Resection of more than one entire vertebra and adjacent discs. Grade 5 resection and additional adjacent vertebral resection
A (anterior release)
P (posterior approach only)
A/P (both)
22.3 Posterior Column Osteotomies (Grades I and II)
For patients with flexibility of the disc spaces, a series of posterior column osteotomies can achieve significant deformity correction. In the realm of open surgery, these osteotomies are typically described as a Smith Peterson or Ponte osteotomy. The essence of the technique involves removal of sufficient spinous process, lamina, and facet bone to allow compression posteriorly between pedicle screws with the axis of sagittal rotation centered on the posterior vertebral body. This stretches the anterior longitudinal ligament and expands the anterior disc.
A single-level osteotomy will yield between 3° and 5° of lordosis. As such, posterior column osteotomies would typically be performed at three or more consecutive vertebral levels and can be used in the thoracic and/or lumbar spine. Since the adult population typically presents with scoliosis or kyphoscoliosis, these osteotomies would preferentially be compressed on the convexity of a scoliosis. An open surgery allows for bilateral osteotomies in the thoracic and/or lumbar spine. For minimal access surgery, no option yet exists for thoracic posterior column osteotomies. However, in the lumbar spine multilevel MIS TLIF, surgery can achieve unilateral facetectomies. When combined with interbody height restoration, this approach can lead to meaningful deformity correction, even in a rigid spine (Figs. 22.1 and 22.2).
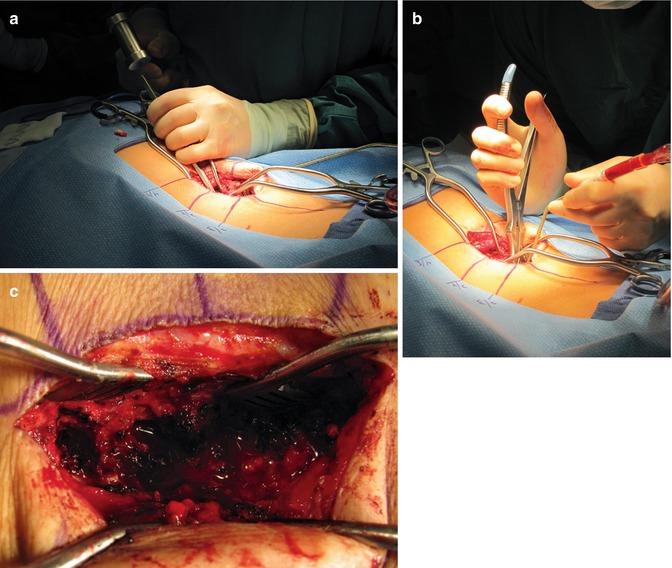
Fig. 22.1
 Costs of Minimally Invasive Spine Surgery
Costs of Minimally Invasive Spine Surgery
 Sagittal Balance
Sagittal Balance
 Lumbopelvic Parameters
Lumbopelvic Parameters
 Presacral Approach for Discectomy and Interbody Fusion in the Setting of Minimally Invasive Spine Surgery Deformity Correction
Presacral Approach for Discectomy and Interbody Fusion in the Setting of Minimally Invasive Spine Surgery Deformity Correction
 Complications of the Lateral Lumbar Transpsoas Approach
Complications of the Lateral Lumbar Transpsoas Approach
 Minimally Invasive Wiltse Approaches for Posterolateral Fusion
Minimally Invasive Wiltse Approaches for Posterolateral Fusion




A mini-open unilateral approach allows the surgeon to access multiple facet joints of interest while preserving much of the dorsal musculature and ligamentous attachments. (a) An osteotome or (b) Leksell rongeur can then be used to remove the facet joint efficiently at (c) multiple levels
Related posts:
Costs of Minimally Invasive Spine Surgery
Sagittal Balance
Lumbopelvic Parameters
Presacral Approach for Discectomy and Interbody Fusion in the Setting of Minimally Invasive Spine Surgery Deformity Correction
Complications of the Lateral Lumbar Transpsoas Approach
Minimally Invasive Wiltse Approaches for Posterolateral Fusion
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
