Chapter 153 Minimally Invasive Posterior Cervical Foraminotomy and Microdiscectomy
Posterior cervical foraminotomy and microdiscectomy is a safe and effective procedure that can be used in the treatment of clinically significant foraminal stenosis resulting from lateral disc herniation or osteophytes. Symptoms improve in more than 90% of patients who undergo the procedure (Fig. 153-1).1–8 Until the late 1950s, this was the predominant approach used in the treatment of herniated cervical discs. In 1958, however, Cloward9 introduced an anterior approach to cervical discectomy, and popularity with this technique grew as modifications to the technique made it safe and easier to perform. In addition, patients experienced less postoperative pain and muscle spasm, they had shorter hospital stays, and surgery could be performed through a smaller incision with less muscle trauma.

Numerous series show that patients achieve good relief from their symptoms with the anterior approach.9–12 However, despite these advantages, the anterior approach is associated with the risk of numerous complications, including recurrent laryngeal nerve injury,13–16 dysphagia and speech dysfunction,17 esophageal injury,18 and airway compromise,19–21 as well as injury to the carotid artery22 and jugular vein.23 In addition, anterior cervical discectomy has been implicated in both radiographic24 and clinically significant adjacent segment degenerative disease,25 as well as altering the native biomechanics of the cervical spine that may result from discectomy and fusion.26,27
Because the posterior approach avoids a complete discectomy and fusion, it remains a viable option in the treatment of lateral soft discs or osteophytes in the cervical region, and superb decompression of the lateral recess and neural foramen has been well documented using posterior laminoforaminotomy.1–5 This approach offers direct visualization of the exiting nerve root and avoids fusion, as is the case with anterior surgery.
Enthusiasm for the posterior approach is tempered by technical limitations that limit visualization of the distal foramen, in addition to generous bony and epidural venous bleeding. Significant muscle dissection also is necessary to obtain adequate surgical exposure, which increases intraoperative bleeding, as well as postoperative pain, muscle spasm, and hospital stay. Also, muscle denervation and retraction injury, as a result of stripping muscles from their point of attachment to the spine, recently have been shown to result in compromised biomechanical stability in the posterior cervical region.28 Negative long-term effects similar to those that may occur with muscle injury during lumbar spine surgery29–32 may also occur with muscle dissection during the approach to the posterior cervical spine.
As a result, posterior microendoscopic foraminotomy (MEF) was developed by Roh et al. to address cervical nerve root compression by direct visualization of pathology while minimizing tissue destruction upon exposure.33 Muscle and ligamentous attachments to the spine are preserved, thus decreasing postoperative pain and spasm and helping maintain long-term stability. Finally, fusion and its associated sequelae are avoided.
Initial cadaveric studies using this technique demonstrated that the average vertical and transverse diameter of the laminotomy defect was identical for MEF or open techniques.33 The average amount of facet removed and the extent of neural decompression was greater with MEF than with the open approach. Initial clinical results were quite favorable for the MEF procedure. Overall, the operative time, blood loss, length of hospitalization, and need for postoperative pain medications were all reduced with the MEF group compared with a similar group of patients who underwent the open procedure.34 Within the MEF group, although some surgeons35 advocate the prone position, we have found that changing from a prone to a semisitting position further improved these variables; compared with the open group, average operative time was reduced from 171 to 90 minutes and average blood loss was lowered from 246 to 28 ml. Moreover, the average hospital stay was reduced from 68 hours in the open group to 8 hours in the sitting MEF group.34 Recently, many series of MEF have shown similar results.33,36–40
We previously described our technique for performing a minimally invasive posterior cervical foraminotomy.41 As described here, lateral soft disc herniations can be treated using the MEF technique by performing a small resection of the superior medial pedicle, thereby allowing access to the herniated disc fragment. Over the last several years, we have preferred to use a microscope instead of an endoscope, because the microscope affords three-dimensional visualization of the anatomy as opposed to the endoscope, which is two dimensional. Other advantages of using the microscope over the endoscope include familiarity among neurosurgeons and improved optics for enhanced visualization of the operative field.
Positioning
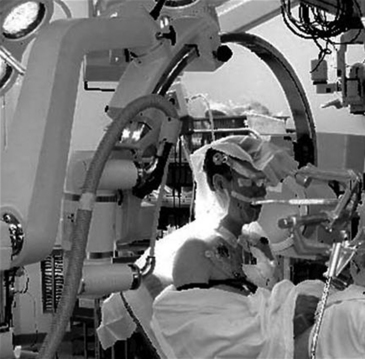
Initially in the supine position, the patient’s head is affixed to the Mayfield head holder, and the patient’s body is gradually brought to a semisitting position such that the knees are level with the heart. The Mayfield adaptor is attached to the table between the hips and the knees and arched back as necessary to accommodate the patient’s body habitus, connecting to the Mayfield head holder. Care is taken to maintain the neck in a comfortable, neutral position. The surgeon should be able to pass two fingers below the chin to assure adequate venous drainage via the jugular veins. The arms are folded and secured across the chest or supported at the sides; pressure points are padded to prevent nerve palsies and pressure sores (Fig. 153-2). Precordial Doppler monitoring is used to monitor air emboli in the right atrium; a central venous catheter is usually not necessary because of the brevity and minimal blood loss associated with the procedure.
Localization
The fluoroscope is positioned to obtain a lateral view of the cervical spine. The midline is marked before drapes are applied by palpation of the spinous processes. The back of the neck is then prepped and draped in a routine surgical fashion. An 18-gauge spinal needle is used to identify the proper level approximately 1.5 cm lateral to the midline. A skin incision is then made over the level of interest. A small retractor is placed to visualize the fascia, and the fascia is cut in a rostral to caudal direction parallel to the spinous processes to expose the underlying muscle. In individuals with large necks, the spinous process can be palpated with a finger to help orient the location of the midline structures. In heavy patients or those with muscular shoulders, the lower levels of the cervical spine can be difficult to visualize. In these cases, the shoulders can be taped down to aid in visualization.
Approach
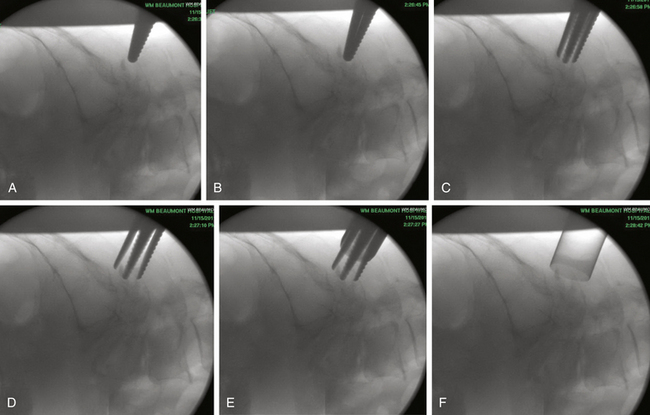
Under fluoroscopic guidance, a Kirschner (K) wire is carefully advanced toward the laminar facet junction. Care needs to be taken so that the K wire is not directed medially, where it can enter the interlaminar space and cause a spinal cord injury. It is therefore imperative to visualize the K wire and dilators as they approach the spine to prevent neurologic injury. In large, muscular individuals, we often stop advancing the K wire before docking on the facet and then pass the first muscle dilator, remove the K wire, and place subsequent muscle dilators and finally the tubular retractor, as shown in Fig. 153-3. Recent developments have resulted in minimal invasive muscle dilators that do not require a K-wire and subsequent muscle dilators to approach the spine (Fig. 153-4). This retractor system might help reduce iatrogenic neural injury.
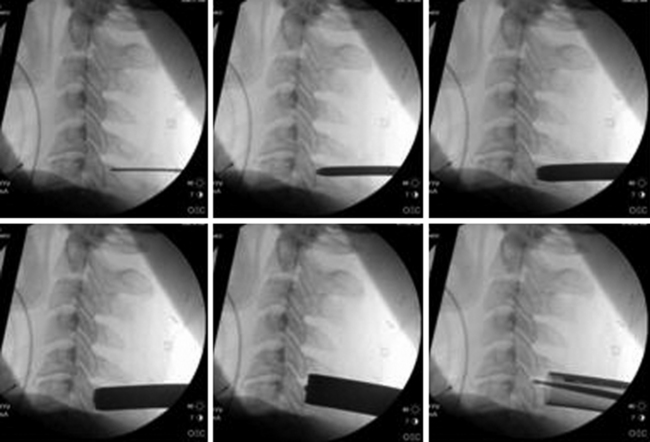
FIGURE 153-3 These images illustrate progressive dilation of the soft tissue in order to create a working channel. This process begins with insertion of a K-wire (top left), and ends with the placement of the tubular retractor (bottom left). A straight curette is seen in the tubular retractor in the bottom left image, and is used to assist in docking onto the lamino-facet complex as described in the text and as seen in Figure 153-4.
< div class='tao-gold-member'>
Related posts:
 Cortical and Subcortical Brain Mapping
Cortical and Subcortical Brain Mapping
 Radiation Therapy and Radiosurgery in the Management of Craniopharyngiomas
Radiation Therapy and Radiosurgery in the Management of Craniopharyngiomas
 Surgical Management of Intracerebral Hemorrhage
Surgical Management of Intracerebral Hemorrhage
 Neurovascular Decompression in Cranial Nerves V, VII, IX, and X
Neurovascular Decompression in Cranial Nerves V, VII, IX, and X
 Role of Gamma Knife Radiosurgery in the Management of Arteriovenous Malformations
Role of Gamma Knife Radiosurgery in the Management of Arteriovenous Malformations
 Arachnoid, Suprasellar, and Rathke’s Cleft Cysts
Arachnoid, Suprasellar, and Rathke’s Cleft Cysts
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


