, Michelle M. Falcone2, Michael Y. Wang2 and Steven Wu1
(1)
Department of Neurosurgery, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA, USA
(2)
Department of Neurological Surgery, University of Miami, Jackson Memorial Hospital, Miami, FL, USA
Abstract
Adult spinal deformity (ASD) refers to an abnormal spinal curvature in the coronal, axial, and sagittal plane in adult patients. Most ASDs are de novo degenerative deformities that are caused by asymmetric disc and facet degeneration or osteoporotic spine insufficiency fracture [20]. Recent publications have indicated that the prevalence of any radiographic evidence of ASD can be as high as 60 % in adults older than 60 years of age [19, 24] and symptomatic scoliosis is seen in 6–30 % of the elderly population. Patients with ASD most commonly seek treatment due to pain and disability from the deformity and its associated disc degeneration, spinal stenosis, nerve roots compression, lateral listhesis, spondylolisthesis, and the overall loss of spinopelvic balance. Most symptomatic ASD patients are initially treated with conservative measures such as physical therapy, nonsteroidal anti-inflammatory medication, and narcotic analgesics. When conservative treatment fails, operative procedures aiming to decompress lumbar nerve roots and the thecal sac stabilize unstable motion segments, reestablish global spinal balance in all planes, and prevent deformity progression are indicated.
18.1 Introduction
Adult spinal deformity (ASD) refers to an abnormal spinal curvature in the coronal, axial, and sagittal plane in adult patients. Most ASDs are de novo degenerative deformities that are caused by asymmetric disc and facet degeneration or osteoporotic spine insufficiency fracture [20]. Recent publications have indicated that the prevalence of any radiographic evidence of ASD can be as high as 60 % in adults older than 60 years of age [19, 24] and symptomatic scoliosis is seen in 6–30 % of the elderly population. Patients with ASD most commonly seek treatment due to pain and disability from the deformity and its associated disc degeneration, spinal stenosis, nerve roots compression, lateral listhesis, spondylolisthesis, and the overall loss of spinopelvic balance. Most symptomatic ASD patients are initially treated with conservative measures such as physical therapy, nonsteroidal anti-inflammatory medication, and narcotic analgesics. When conservative treatment fails, operative procedures aiming to decompress lumbar nerve roots and the thecal sac stabilize unstable motion segments, reestablish global spinal balance in all planes, and prevent deformity progression are indicated.
ASD Surgery can be very rewarding for patients, yielding significant improvements in back and leg pain. This has been proven in previous studies utilizing objective quality-of-life (QOL) measures like the Scoliosis Research Society 22 questionnaire (SRS-22) and Oswestry Disability Index (ODI) [5, 32, 33]. Nevertheless, adult deformity surgeries are highly complex and require prolonged anesthesia, a long recovery period, and extended hospital stay. Traditional open deformity surgeries are associated with high rate of serious complications, and it has been reported that open deformity surgeries have major complication rates as high as 40 %. In a series of 361 patients who underwent open deformity surgery, Pateder and colleagues reported that the 30-day mortality rate was 2.4 % [23]. In 2011, Smith et al. analyzed data from the Spinal Deformity Study Group and reported that 26.2 % of their 206 patients suffered a minor complication and 15.5 % suffered a major complication [31]. Staged procedures or combined anterior-posterior approaches have also been found to be associated with higher complication rates [26]. Interestingly, despite the fact that elderly patients were found to have higher perioperative complication rates as high as 71 %, they had the greatest improvement in pain and disability with surgery [34].
One of the major goals of deformity surgery is to restore the coronal and sagittal balance of the spine. Traditionally, deformity surgery has been focused on correcting coronal imbalance. However, global sagittal balance has more recently been found to be more relevant in patient’s symptom and surgical outcome. Glassman et al. reviewed a prospective adult spinal deformity case series with correlated radiographic measures and found that sagittal balance was the most reliable predictor of clinical symptoms [11]. Patients with positive sagittal balance and inadequate lumbar lordosis have worse physical and social function and pain. In these patients, restoration of global sagittal alignment is necessary for significant symptom improvement and pseudoarthrosis avoidance [4, 25].
In traditional open deformity surgery, a variety of techniques have been used to enhance lumbar lordosis and restore sagittal balance. Multilevel anterior lumbar interbody fusion (ALIF) has been demonstrated to be an effective method to achieve normal lumbar alignment [9, 15, 36]. Placement of an anterior graft allows distraction of the anterior disc space, increases disc space height, and improves lumbar lordosis. The large graft size used with an anterior approach also enhances construct stability. The drawback of using ALIF for lumbar alignment is the need for a two-stage surgery, which subjects patients to increased anesthesia time, higher complication rates, and additional approaches.
Rigid sagittal imbalance corrections are most often achieved with pedicle subtraction osteotomy (PSO) in adult deformity surgery [13, 18, 21, 27]. However, PSO is frequently associated with high volume of blood loss and high surgical morbidity and complications [6]. The amount of bony and soft tissue resection required in pedicle subtraction osteotomy also limits its use in minimally invasive surgery (MIS) [39].
The recently developed MIS lateral transpsoas interbody technique has been adopted with much enthusiasm in less invasive deformity surgery. This technique has been shown to be excellent in treating local degenerative arthritis, restoring foraminal height, achieving indirect neural decompression, and correcting coronal deformity [22, 29]. However, the lateral transpsoas approach has been shown to be less effective in treating sagittal imbalance and restoring lumbar lordosis. In a recently reported series of 35 patients by Acosta et al., the lateral transpsoas approach allowed a coronal Cobb angle correction from 21.4° preoperatively to 9.7° postoperatively, a statistically significant improvement. However, lumbar lordosis only changed from 42.1° to 46.2°, despite improvement in interbody height. Overall, the global sagittal alignment was unchanged [1]. These results are similar to the 5° improvement in global lordosis noted by Karikari et al [17]. Modification of the technique by adding the resection of the anterior longitudinal ligament (ALL) has been proposed to enhance sagittal correction allowed with the lateral approach [2, 7, 8, 37]. However, resecting the ALL blindly has the inherent risk of seriously injuring the great vessels. Furthermore, in adult degenerative patient hypertrophied facet joints and stiff posterior elements limited the amount of sagittal correction that can be achieved with the release of anterior elements. More importantly, the majority of physiological lumbar lordosis is found at the L5–S1 and L4–L5 levels, which are problematic to access or with the direct lateral approach.
18.2 Use of Open Multilevel TLIF for Coronal and Sagittal Deformity Correction
Jagannathan et al. published a report in 2009 demonstrating the efficacy of using multilevel TLIF to restore lumbar sagittal alignment [16]. In this retrospective study, 80 patients who had received short-segment (1, 2, or 3 level) transforaminal lumbar interbody fusion (TLIF) procedures for lumbar degenerative disorders were studied. Bilateral facetectomies with interspinous distraction were used so that a large-size boomerang-shaped graft could be placed at the anterior part of the disc space. After insertion of the interbody graft and placement of the pedicle screws, the construct was compressed. At follow-up, radiographic studies demonstrated effective increase of focal lordosis at each of the surgical levels performed. L5–S1 and L4–L5 TLIFs were most effective in restoring segmental lumbar lordosis. An average of 22.2° of segmental lordosis improvement was achieved with a L5–S1 TLIF, and L4–5 TLIF was associated with an average of 11.3° improvement. Multilevel TLIF was more effective in correcting overall lumbar lordosis than single-level surgery (27.3° +/− 3.4° vs. 17.4° +/4.4°). For the majority of patients with a preoperative sagittal imbalance of less than 10 cm, short-segment TLIF procedures were able to improve sagittal alignment. However, only 30 % of the patients with a sagittal imbalance of more than 10 cm achieved acceptable restoration, indicating the need for a more extensive surgery such as osteotomy procedures with long-segment fusion. Yson et al. also published a similar series using multilevel TLIF with bilateral facet resection for segmental lumbar sagittal correction. Similar methods of bilateral facet resection and the use of an interbody spacer placed as anterior as possible were applied demonstrating that significant lordosis restoration can be achieved using multilevel TLIF [40].
The position and the geometry of the cage significantly influence the effect of the sagittal correction after TLIF [10, 12]. In the past several publications had described the TLIF as a procedure that could reduce lumbar lordosis [9, 15]. This was likely due to the specific surgical techniques used. In both series by Jagannathan and Yson, the use of large anteriorly placed spacers helped restore of the lumbar lordosis, similar to the cantilever TLIF procedure described by Anand et al [3]. More importantly, the bilateral facetectomies, the radical discectomy to allow sufficient segmental mobilization, and final compression of the pedicle screws allowed significant restoration of lumbar lordosis.
Heary and Karimi described using unilateral placed TLIF cage for coronal balance correction [14]. In their series of four patients, TLIF cages were placed unilaterally on the concave side, and bilateral facetectomies were used to release the rigid curve. The selective applications of the increased compressive forces were used on the convex side of the construct. Mean correction of the coronal curve of 17.9° was achieved in the small series.
18.3 The Use of MIS Multilevel MIS TLIF in Adult Deformity Surgery
MIS TLIF has been widely used over the past decade to address degenerative lumbar disc disease, spondylolisthesis, and recurrent lumbar disc herniations [28]. Since open multilevel TLIF has been shown to correct sagittal imbalance efficiently, it stands to reason that multilevel MIS TLIF could be a promising approach for MIS deformity surgery, without subjecting patients to multiple stage surgeries since the whole surgery is performed with the patient in prone position. Wang published his experience using multilevel MIS TLIF with expandable cages in a series of 25 adult spinal deformity patients [38]. This case series utilized expandable interbody cages to restore anterior column height combined with percutaneous pedicle screw fixation. An average of 3.2 interbody levels were treated in these patients. The mean preoperative Cobb angle was 29.2°, improving to 9.0° postoperatively; the mean preoperative global lumbar lordosis was 27.8°, improving to 42.6° postoperatively; and the mean preoperative SVA improved from 7.4 cm to 4.3 cm postoperatively. Clinically, at 1-year follow-up, the NPS for leg pain improved from 5.1 to 1.8 after surgery, and the NPS for back pain improved from 7.6 to 3.4. The ODI score improved from 44.9 to 24.1 after surgery.
18.4 Surgical Technique
1.
Positioning: The surgery is performed after induction of general anesthesia with the patient lying prone. Positioning on the Jackson table is critical to allow the belly to hang and to increase lordosis, as it has been shown that the use of Jackson table enhances postoperative lumbar lordosis [35].
2.
Skin Incision: For long-segment minimally invasive deformity surgery, it is more cosmetically pleasing to use a single midline incision. The principle of minimally invasive surgery is not the size of the skin incision but the minimal disruption of normal soft tissues and bony structures to achieve the desired outcome. A single midline incision with preservation of the fascia plane is minimally disruptive and cosmetically pleasing with better wound healing than multiple bilateral stab incisions. Furthermore, many patients already have had a previous surgery with a midline lumbar scar.
3.
Development of the Suprafascial Plane: After making the skin incision with meticulous hemostasis, a plane is developed above the superficial fascia so that percutaneous screws can be placed and the TLIF corridor can be accessed with minimal disruption of the soft tissue envelope (Fig. 18.1).

Fig. 18.1
Single midline incision and the development of the subskin fascia plane
4.
 Classification Schema for Scoliosis
The Importance of the Fractional Curve
Presacral Approach for Discectomy and Interbody Fusion in the Setting of Minimally Invasive Spine Surgery Deformity Correction
MIS in Adolescent Deformity
Minimally Invasive Thoracolumbar Facet Joint Fusion
Minimally Invasive Cement-Augmented Pedicle Screw Fixation
Classification Schema for Scoliosis
The Importance of the Fractional Curve
Presacral Approach for Discectomy and Interbody Fusion in the Setting of Minimally Invasive Spine Surgery Deformity Correction
MIS in Adolescent Deformity
Minimally Invasive Thoracolumbar Facet Joint Fusion
Minimally Invasive Cement-Augmented Pedicle Screw Fixation




Access Corridor: At this time, traditional MIS TLIF with fixed or expandable tubes can be used for performing the TLIF procedures. We often elect to perform multilevel TLIF in a mini-open fashion by performing subperiosteal dissection only on the side of the interbody access. Only one side of the spine is accessed to allow for facetectomies and interbody cage placement. With the preservation of muscle attachments to the spine on the contralateral side, patients generally have a much faster recovery time and less postoperative pain than traditional bilateral open procedures (Fig. 18.2). The unilateral subperiosteal dissection is taken to the lateral facet joints, and a retractor is used to maintain the opening.
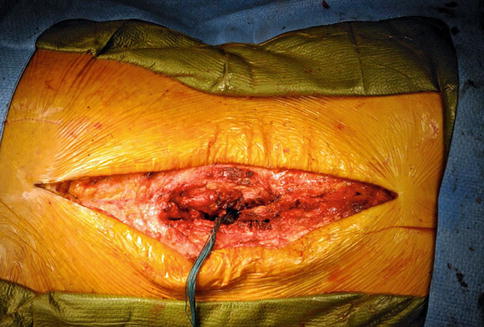
Fig. 18.2
The amount of tissue dissection for mini-open deformity surgery
Related posts:
Classification Schema for Scoliosis
The Importance of the Fractional Curve
Presacral Approach for Discectomy and Interbody Fusion in the Setting of Minimally Invasive Spine Surgery Deformity Correction
MIS in Adolescent Deformity
Minimally Invasive Thoracolumbar Facet Joint Fusion
Minimally Invasive Cement-Augmented Pedicle Screw Fixation
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
