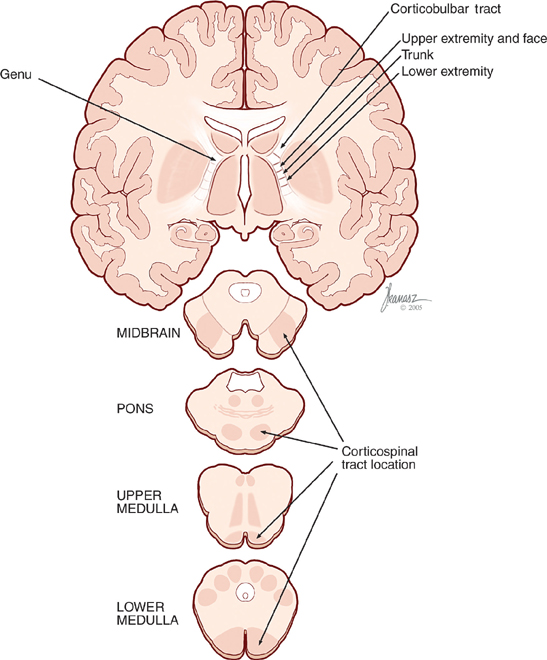
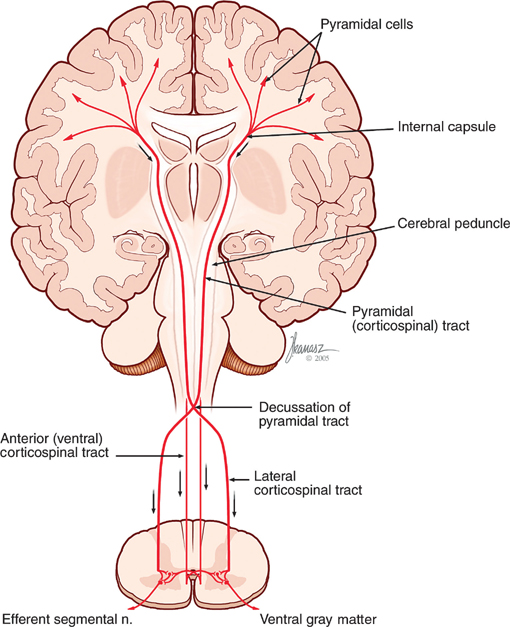
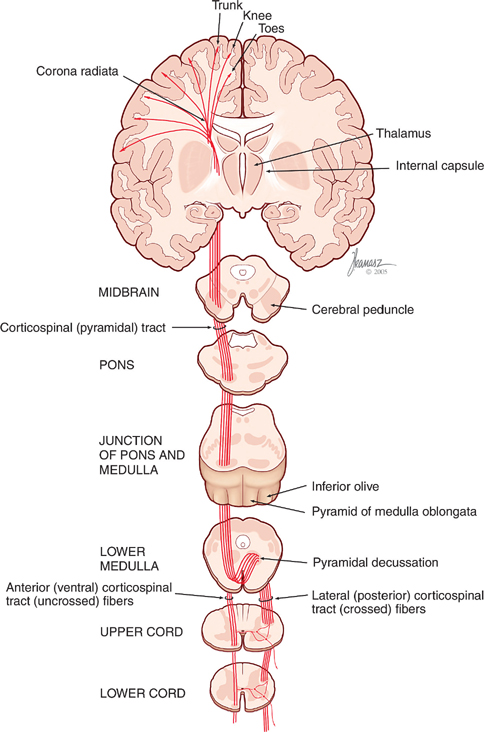
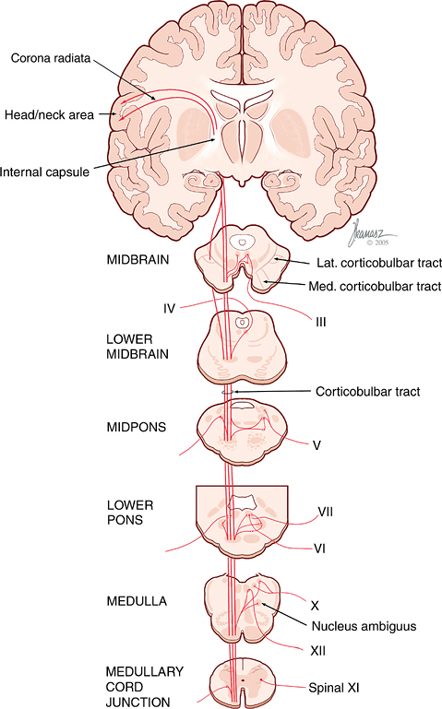
19 Motor System The motor system is complex and has many components. The system is composed of both supraspinal and spinal pathways. These may be further broken down into pathways that begin in the cortex and the brainstem. Moreover, there are cortical and subcortical regions of the brain that are concerned with higher order control of the descending pathways. This chapter presents a description of the anatomic integration of these components, as well as the neurologic implications. Fig. 19.1 Subcortical and corticospinal pathways. See Figs. 19.1 and 19.2. The corticospinal (pyramidal) tract drives skilled and precise movement of the upper and lower extremities. Its mechanism of action is via the contraction of individual muscles. The tract begins in the precentral gyrus (primary motor cortex, Brodmann’s area 4). The primary motor cortex is arranged somatotopically. Stimulation of the primary motor cortex results in individual muscle contractions. These contractions, however, are only a small aspect of complex movements. Other regions of the cortex (i.e., premotor cortex) are involved in and help coordinate complex muscle activity (see later discussion). The corticospinal tract is composed of ~1 million fibers. Approximately 30% arise from lamina V of the primary motor cortex, 30% from the premotor cortex, and 40% from the parietal lobe (sensory). Fig. 19.2 Corticospinal tract. See Fig. 19.3. Axons leaving the cerebral cortex descend toward the brainstem by way of the corona radiata. They then converge and descend into and through the posterior limb of the internal capsule. The fibers in the posterior limb of the internal capsule are arranged topographically, with those of the upper extremity located in the rostral part and those of the lower extremity located more caudally. Axons then pass through and form the cerebral peduncles of the midbrain along with other descending cortical fibers. The pyramidal fibers remain distinct and occupy the middle two thirds of the peduncles. Axons continue on as the descending pyramidal tract through the pons and form the pyramids on the ventral aspect of the medulla. In the lower medulla, ~90% of the fibers of the pyramids decussate. The decussated fibers then form the lateral cor-ticospinal tract in the lateral funiculus of the spinal cord. These neurons are termed upper motor neurons. This terminology is important to note when evaluating a patient with motor weakness (see later discussion). The upper motor neurons of the lateral corticospinal tract descend through the lateral funiculus of the spinal cord. At the appropriate levels, motor neurons (seated in the ventral gray matter) extended axons (lower motor neurons) to innervate the extremity vasculature. These motor neurons receive input from descending axons in the spinal cord. The synapse, from upper to lower motor neuron, is rarely direct (only in ~10% of cases). More often than not, there is a connection with interneurons in the intermediate spinal laminae prior to synapse with the lower motor neuron. As previously mentioned, several corticospinal fibers do not cross at the lower medulla and descend uncrossed in the ventral funiculus as the anterior corticospinal tract. The lower motor neuron (alpha motor neuron) is located in the nuclei of the medial (trunk) and lateral (extremity) portions of the ventral gray matter. The lower motor axons exit through the ventral roots and help form the spinal nerves at the appropriate levels. They then innervate the skeletal muscles of the trunk and extremities. Fig. 19.3 Corticospinal tract, axial view. Similar to the corticospinal tract anatomically and in function, the corticobulbar tract contributes to cranial nerve innervation, providing supply to the muscles of facial expression and mastication and the tongue. See Fig. 19.4. Fibers leave the cortex (primary motor cortex) and converge and descend through the corona radiata, the anterior portion of the posterior limb of the internal capsule, and into the brainstem. The tract continues though the cerebral peduncle of the midbrain, occupying the middle two thirds. In the brainstem, axons of the corticobulbar tract exit some distance above their respective cranial nerve nuclei and synapse on interneurons in the reticular formation. They may travel in the reticular formation, medial longitudinal fasciculus, and medial lemniscus to reach their cranial nerve nuclei. The majority of the cranial nerve nuclei are innervated by both crossed and uncrossed fibers. Therefore, when one fiber is injured, innervation from the uninjured side (either crossed or uncrossed) still exists, and a deficit may not be observed. An important exception to this is the facial nucleus. The portion of the facial nucleus that innervates the lower facial muscles is supplied by crossed upper motor neuron fibers only, whereas those that subserve the upper facial muscles receive both crossed and uncrossed fibers. Thus, an injury to the corticobulbar tract will result in contralateral weakness of the lower facial muscles, leaving the upper facial muscles intact. Fig. 19.4 Corticobulbar tract. Several extrapyramidal motor tracts originate in the brainstem. The purpose of these tracts is to maintain muscle tone, posture, balance, and reflex movement. They are under supraspinal control, and their action is not at the conscious level. Injury may lead to disinhibition of these tracts and abnormal posture and tone. There are two components of the reticulospinal tract system. These are the pontine and medullary reticulospinal tracts. The pontine reticulospinal tract is thought to be an excitatory tract that innervates motor neurons supplying the axial and limb muscles. Its greatest effect is on the axial muscles in the neck. The medullary reticulospinal tract is an inhibitory tract. It may act to keep other facili-tatory and inhibitory tracts in check and is under cortical control. Loss of cortical control, as with upper brainstem injury, is a component of the constellation of neural alterations that contribute to extensor (decerebrate) posturing. See Fig. 19.5. The tract arises from cells in the pontine tegmentum. It descends ipsilaterally in the medial anterior funiculus traversing the length of the spinal cord, and in the process sending many branches to multiple spinal levels.
Cortex
Corticospinal Tract
Course of the Corticospinal Tract
Corticobulbar Tract
Course of the Corticobulbar Tract
Brainstem
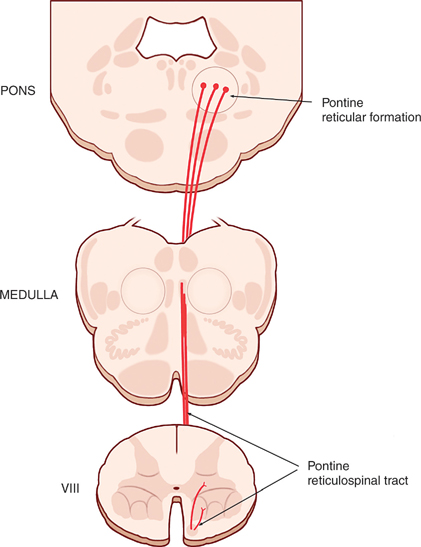
Reticulospinal Tract
Course of the Pontine Reticulospinal Tract
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


