Chapter 167 Percutaneous Placement of Lumbar Pedicle Screws
Indications and Techniques
Introduction
The use of pedicle screws for spinal stabilization has become increasingly popular worldwide. Pedicle screw systems engage all three columns of the spine and can resist motion in all planes. Several studies suggest that pedicle screw fixation is a safe and effective treatment for many spinal disorders.1,2 Standard techniques for pedicle screw placement, however, require extensive tissue dissection to expose entry points and to provide a lateromedial orientation for optimal screw trajectory. Open pedicle fixation and spinal fusion have been associated with extensive blood loss, lengthy hospital stays, and significant cost.3 Minimally invasive placement of pedicle screws can potentially address these issues without compromising the accuracy of placement.4
The use of percutaneous lumbar pedicle screws and an interconnecting subfascial rod was first described in 20015 and later adopted by others.6,7 The spinal implants used for percutaneous pedicle screw fixation are essentially the same as those used in conventional open techniques. To preserve soft tissue and allow for safe and effective insertion of these implants into the lumbar spine, certain principles need to be followed. For example, the pedicle screws are commonly placed over K-wires. These allow the surgeon to gain access to a pedicle pilot hole with minimal, if any, direct visualization. Screw extenders, which allow for percutaneous manipulation and localization of the screws once they have been inserted and cannot be seen directly by the surgeon, also provide a means for screw alignment so that an interconnecting rod can be successfully joined to the screws in a minimally invasive fashion. This chapter describes techniques for percutaneous lumbar pedicle screw fixation and the present related outcome data.
Operative Techniques
Patient Positioning and Operating Room Setup
Percutaneous pedicle fixation of the lumbar spine can be performed after induction of general or epidural anesthesia. Thereafter the patient is positioned prone on top of a radiolucent spinal surgery table with the abdomen free. Chest rolls on a radiolucent flattop or Jackson-type frame can be used for this purpose. For guidance during percutaneous screw placement, options include conventional fluoroscopy, virtual fluoroscopy, or intraoperative CT-based imaging. Regardless of whether one uses conventional or virtual fluoroscopic guidance during the procedure, it is important to check that adequate anteroposterior (AP) and lateral fluoroscopic images of the lumbar spine can be obtained before preparing and draping the patient.
Initial Incision and Pedicle Identification
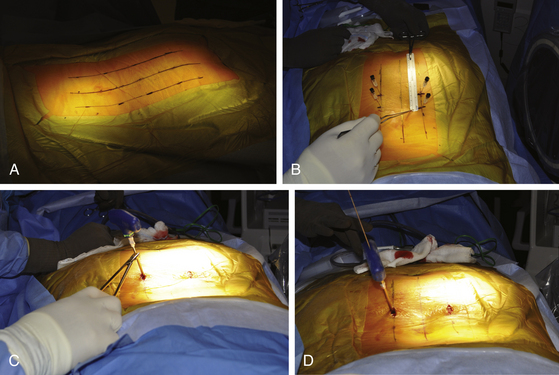
Fluoroscopic images are obtained in the AP and lateral planes to ensure that the pedicles can be adequately visualized. If necessary, oblique (or “owl’s-eye”) views can be obtained as well. It is important that “true” AP and lateral views are obtained because even a minor misalignment in imaging may lead to wayward screw placement. To ensure a true AP view, the spinous process must lie precisely in the center of the interpedicular space. To obtain a true lateral view, the pedicles should overlie one another and the end plates should be linear (not elliptical). If the patient is scoliotic, the C-arm should be angled to achieve these views. Furthermore, to avoid parallax, center the target anatomy on the fluoroscopic screen. It is therefore important to check the fluoroscopic views before the skin is prepared and the patient is draped. This allows for manipulation and repositioning of the patient, bed, and fluoroscopic C-arm without compromising the sterile field. Additionally, the use of a radiolucent table (e.g., Jackson table) and, if used, a radiolucent positioning device (e.g., gel chest rolls) is important. A small incision is made approximately 4 to 5 cm off the midline, depending on the size of the patient (Fig. 167-1A). For a thin patient, an incision 4 cm off the midline is utilized. A more lateral incision is made for an obese patient. The principle is that a lateromedial trajectory is desired; the object is to maximize the bone purchase of the pedicle screw while avoiding the facet complex. A larger patient, with more soft tissue dorsal to the spine, requires an incision that is farther from the midline to achieve the same trajectory as that for a thinner patient. A 22-gauge spinal needle can be used to localize the position of the incision prior to cutting the skin (Fig. 167-1B). The incision length is dependent on the diameter of screw extenders but is approximately 1.5 cm for a single screw and 2.5 cm for two screws.
Pedicle Screw Placement
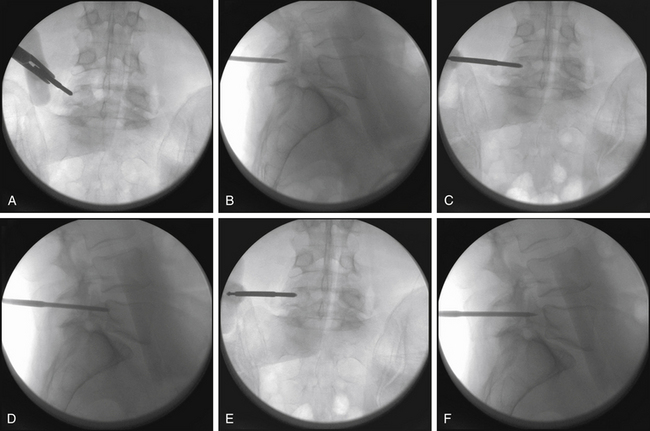
Thorough knowledge of pedicle anatomy and the sagittal and axial angulation of the individual pedicles is mandatory for safe percutaneous screw placement.8 These angles are best judged using preoperative CT or MRI of the lumbar region. The pedicle can be navigated using a conventional C-arm fluoroscope that is alternated between AP, lateral, and oblique views. One must obtain multiple sequential views of the pedicle probe in at least two planes as it is advanced down the pedicle.1,8 It is important to keep these trajectories in mind to ensure the accuracy of percutaneous screw placement. The ideal pedicle entry point is at the base of the transverse process as it joins the superior articular process; this location allows for the lateromedial trajectory of screws and minimizes the anatomic disturbance of the facet joint. One advantage of percutaneous screw placement over the conventional open technique is that it is much easier to achieve the required medial angulation because extensive soft-tissue and muscle retraction is avoided. A Jamshidi-type needle is used to create a pilot hole under fluoroscopic guidance (Fig. 167-1C and D). The needle is advanced through the pedicle into the vertebral body. Fluoroscopic images of three positions of the Jamshidi needle should be obtained: the initial starting point, the middle position within the pedicle, and the position at the pedicle-vertebral body junction. For the initial starting point, the Jamshidi needle should be coaxial with the pedicle on the lateral fluoroscopic image. The starting AP image should reveal the tip of the needle to be at the lateral border of the pedicle (Fig. 167-2A and B). When lateral fluoroscopy shows the tip of the needle has been advanced to the pedicle-vertebral body junction, the AP image should reveal that the Jamshidi needle tip is just lateral to the medial cortical wall of the pedicle, with approximately 4 mm of space to spare (Fig. 167-2C and D). This ensures that there is adequate room for the subsequent placement of a screw (with a radius of approximately 2.75 to 3.75 mm), thus minimizing the potential for medial wall breach and nerve root irritation. The value of obtaining AP and lateral fluoroscopic views of the needle when it has been advanced approximately one half the way down the pedicle is that course adjustments can still be made (Fig. 167-2E and F). If the tip is still close to the lateral cortical wall of the pedicle on the AP view at this point, the needle trajectory needs to be medialized. If the tip is too close to the medial wall, the needle risks penetrating into the canal as it is advanced and its course needs to be lateralized. Although the surgeon can remove the needle from the pedicle and start over, it is often more efficient to steer the needle tip within bone by switching the needle trochar from a pointed tip to a beveled tip (leaving the needle hub in place). If the bevel is placed in a lateral position, a force vector will push the tip of the needle in a medial direction as it is advanced. In similar fashion, medial placement of the bevel will cause the needle tip to be deflected laterally as it is advanced. Once the needle has been confirmed to be in an acceptable position on the AP and lateral fluoroscopic views at the pedicle-vertebral body junction, the needle is advanced into the vertebral body. A K-wire is inserted through the needle into the cancellous bone of the vertebral body, and the needle is withdrawn (Fig. 167-2D). This K-wire will serve as a “switching stick” for subsequent placement of a tap and screw down the same pedicle pilot hole trajectory (Fig. 167-3).
< div class='tao-gold-member'>
Related posts:
 Cortical and Subcortical Brain Mapping
Cortical and Subcortical Brain Mapping
 Radiation Therapy and Radiosurgery in the Management of Craniopharyngiomas
Radiation Therapy and Radiosurgery in the Management of Craniopharyngiomas
 Surgical Management of Intracerebral Hemorrhage
Surgical Management of Intracerebral Hemorrhage
 Contemporary Dorsal Rhizotomy Surgery for the Treatment of Spasticity in Childhood
Contemporary Dorsal Rhizotomy Surgery for the Treatment of Spasticity in Childhood
 Role of Gamma Knife Radiosurgery in the Management of Arteriovenous Malformations
Role of Gamma Knife Radiosurgery in the Management of Arteriovenous Malformations
 Arachnoid, Suprasellar, and Rathke’s Cleft Cysts
Arachnoid, Suprasellar, and Rathke’s Cleft Cysts
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


