 Figure 41.1 The ascending arousal system. Two major pathways are shown. One (shown in light gray) providing upper brainstem input to the thalamic-relay nuclei and to the reticular nucleus of the thalamus coming from the pedunculopontine and laterodorsal tegmental (PPT/LDT) nuclei, which are acetylcholine (ACh)-producing neuronal groups. The second major group of neurons (shown in dark gray) come from the noradrenergic (NA) locus coeruleus (LC), serotoninergic (5-HT) dorsal and median raphe nuclei, dopaminergic (DA) periaquiductal gray matter (vPAG), and histaminergic (His) tuberomamillary neurons (TMN). Additional cortical input merges from the basal forebrain (BF) neurons containing GABA or ACh, and by lateral hypothalamic (LH) peptidergic neurons that contain melanin-concentrating hormone (MCH) or orexin (hypocretin) (ORX). (Reproduced from Saper CB, Scammell TE, Lu J. Hypothalamic regulation of sleep and circadian rhythms. Nature. 2005; 437:1257-1263, with permission.) |
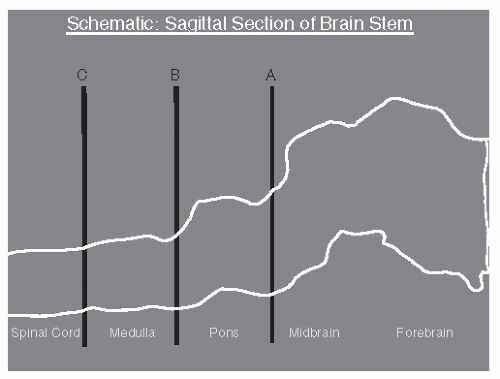 Figure 41.2 Schematic sagittal section of the brainstem of the cat. A: Junction of midbrain and pons. B: Junction of pons and medulla. C: Junction of medulla and spinal cord. (Reproduced from Chokroverty S. Sleep Disorders Medicine: Basic Science, Technical Considerations and Clinical Aspects. 3rd ed. Philadelphia: Saunders/Elsevier; 2009, with permission.] |
Table 41.1 Physiologic Changes during Wakefulness, NREM Sleep, and REM Sleep | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
fruit flies (Drosophila) and mammals has been made (26). Dysfunction of the circadian rhythm results in several important sleep disorders including delayed sleep phase syndrome and advanced sleep phase syndrome.
mattress, a closet, and night stand. The sleeping room should be quiet and sound attenuated so that noises from outside the sleep laboratory and technologist’s area do not disturb the sleeping patient. An intercommunication system for contact with the patient is essential. Toilet facilities should preferably be attached to the bedroom and a shower should also be readily available.
quantification of blood oxygen levels are necessary and accomplished using pulse oximetry. Endoesophageal (intrathoracic) pressure recording is also sometimes used in the detection of partial obstructions or upper airway resistance that can exist without actual apneas or hypopneas. The nasal pressure transducer (NPT) is recommended for the measurement of subtle reductions in airflow and can also be used in the identification of absent airflow, characteristic of apnea.
uses a Stow-Severinghaus glass/ceramic electrochemical sensor, with a small heater unit to facilitate blood flow. Transcutaneous monitoring of CO2 tension is more reliable than transcutaneous measurement of O2 because CO2 diffuses better through the skin.
Table 41.2 Filter Settings for PSG Recordings | ||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
associated with increasing delta activity. Stage N3 is scored when 20% or greater of an epoch is delta activity (Fig. 41.6). For the purposes of sleep scoring, delta activity is defined as activity of 0.5 to 2 Hz that is at least 75 µV in amplitude when measured over the frontal or central regions. Sleep spindles may persist into stage N3, but eye movements are usually absent. Axial EMG is usually lower than stage N2 and may approach that seen in stage R.
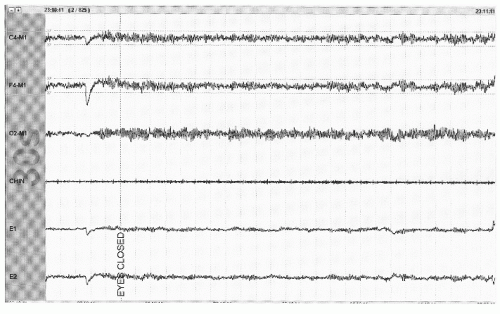 Figure 41.3 The limited PSG montage illustrates alpha activity (well seen after eye closure) consistent with wakefulness or stage W (30-second epoch, chin = submental EMG). |
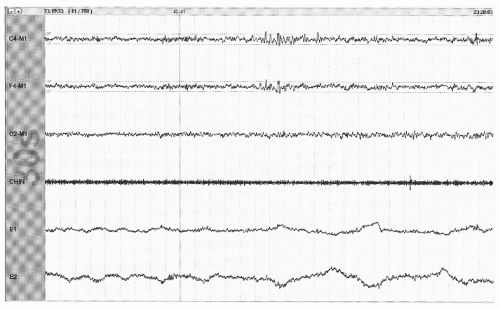 Figure 41.4 The limited PSG montage illustrates the absence of alpha activity and the appearance of slow eye movements (out-of-phase activity in channels E1 and E2) consistent with stage N1 sleep (30-second epoch, chin = submental EMG). |
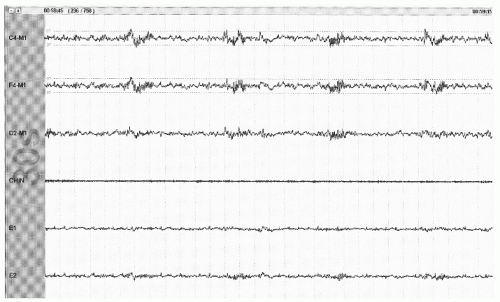 Figure 41.5 The limited PSG montage illustrates sleep spindles (sinusoidal activity in top two channels) and broad vertex waves consistent with stage N2 (30-second epoch, chin = submental EMG). |
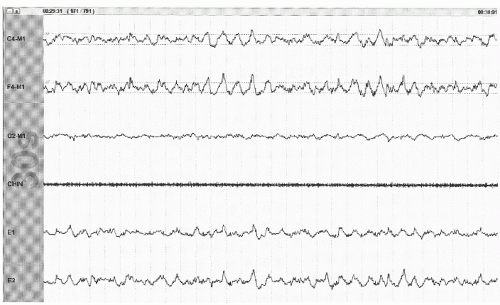 Figure 41.6 The limited PSG montage illustrates high-amplitude delta activity (<2 Hz) occupying greater than 20% of the epoch and represents an example of stage N3. Waveforms that span the two dotted lines in the top two channels identify activity that is at least 75 µV in amplitude (30-second epoch, chin = submental EMG). |
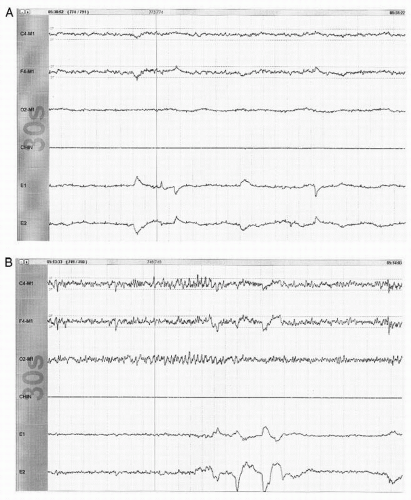 Figure 41.7 A: An example of stage R sleep with low-amplitude mixed frequency EEG activity, absent axial EMG activity (chin channel represents submental EMG), and REMs (out-of-phase activity in channels E1 and E2). (30-second epoch). B: Another example of stage R sleep. Note 2 to 3 Hz low-amplitude sharp activity (seen in C4-M1 channel) just prior to REMs. This activity represents sawtooth waves, a pattern frequently seen in stage R. |
clinical diagnosis made in the clinic based primarily on the history and does not require PSG evaluation. PLMS is a diagnosis made on the PSG as most patients do not have daytime symptoms and observer history is not usually helpful. Most patients with RLS will also have PLMS, but PLMS most commonly occur in the absence of restless legs symptoms. Periodic limb movements in wakefulness (PLMW) are not part of the recently published AASM scoring guidelines (12). However, several investigators have suggested the utility of PLMW in assessing patients with RLS. The scoring criteria are exactly the same as those outlined above for the scoring of PLMS. These investigators have also proposed a SIT test (suggested immobilization test) with associated quantification of PLMW as a diagnostic test for patients with RLS (41).
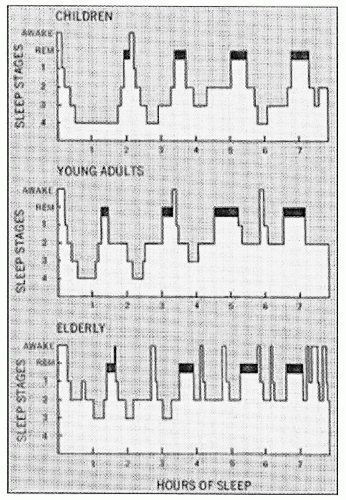 Figure 41.8 Histograms representing normal sleep cycles for age. REM sleep represented by darkened area. Note NREM stages 3 and 4 would now be combined into stage N3. Horizontal axis is hours of PSG recording. (From Kales A, Kales J. Recent findings in the diagnosis and treatment of disturbed sleep. N Engl J Med. 1974;487-499, with permission.) |
 Figure 41.9 Example of arousal from NREM sleep (stage N2) with appearance of fast activity lasting at least 3 seconds. Note increase in EMG activity, which commonly accompanies an EEG arousal pattern but is not required for scoring an arousal from NREM sleep (30-second epoch). |
syndrome consistent with OSA but without scorable apneic events. With the use of NPT and the associated identification of scorable hypopneas, it is much rarer to have a clinical suspicion of unrecognized respiratory events contributing to a patient’s symptoms. However, the NPT is frequently overly sensitive in that it demonstrates no airflow (an apnea) while the thermal sensor continues to demonstrate obvious airflow. As such, the NPT is not to be used for determination of apneic events, which are to be scored off of the thermal sensor recording.
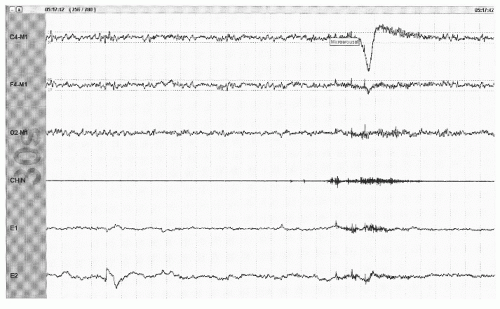 Figure 41.10 An arousal from stage R with appearance of >3 seconds of faster frequencies accompanied by the appearance of EMG in the axial (chin) EMG channel (30-second epoch). |
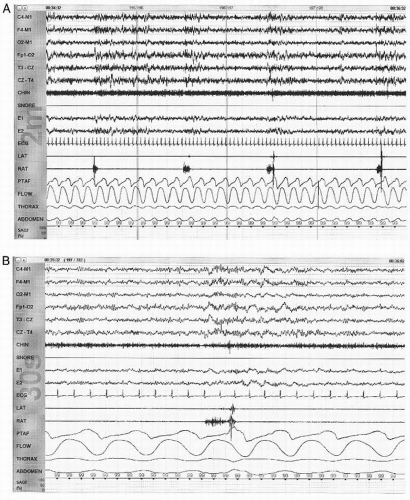 Figure 41.11 A: An illustration of periodic limb movements of sleep. This is a 2-minute epoch with the appearance of EMG activity in the right anterior tibialis (RAT) channel occurring approximately every 30 seconds. The patient is in NREM sleep (which is not able to be confidently determined in this 2-minute epoch). B: A 30-second epoch taken from the time period illustrated in A. Note the appearance of faster frequencies on the EEG demonstrating an arousal associated with this periodic movement. |
NPT signal decreases by >30% for at least 10 seconds.
There is an accompanying oxygen desaturation of 4% or more.
NPT signal decreases by >50% for at least 10 seconds.
There is an accompanying oxygen desaturation of 3% or more or the event is accompanied by an EEG arousal within 3 seconds of the event.
Score sinus tachycardia for sustained sinus heart rate >90 beats per minute.
Score sinus bradycardia for sustained sinus heart rate <40 beats per minute.
Score asystole for cardiac pauses >3 seconds.
Score wide complex tachycardia for a rhythm of at least three consecutive beats at a rate greater than 100 beats per minute and a QRS duration of > 120 msec.
Score narrow complex tachycardia for a rhythm of at least three consecutive beats at a rate >100 beats per minute and a QRS duration of < 120 msec.
Score atrial fibrillation if there is an irregularly irregular ventricular rhythm associated with replacement of consistent P waves with variable rapid oscillations.
Other significant arrhythmias (such as heart block) should be reported if quality of the single lead is sufficient for accurate identification.
gold standard for looking at sleep macrostructure. CAP presents another way of looking at NREM sleep within those sleep stages.
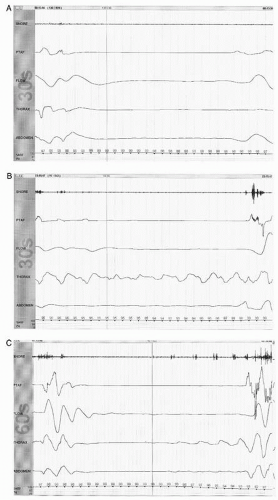 Figure 41.12 A: Limited PSG montage demonstrating no evidence of airflow as measured by nasal pressure transducer (PTAF channel), oronasal thermocouple (flow channel) accompanied by the absence of ventilatory effort in the thorax, and abdominal channels (measured by respiratory inductive plethysmography belts). This is an example of a central apnea lasting approximately 16 seconds. B: Limited PSG montage demonstrating no evidence of airflow as measured by nasal pressure transducer (PTAF channel), oronasal thermocouple (flow channel) accompanied by the evidence of continued ventilatory effort in the thorax channel (measured by respiratory inductive plethysmography belts). This is an example of an obstructive apnea lasting approximately 18 seconds. Note the appearance of snore artifact (in snore and PTAF channel) with resumption of airflow. C: Limited PSG montage demonstrating an apneic event lasting approximately 40 seconds (in this 60-second epoch). No evidence of airflow is noted by the nasal pressure transducer (PTAF channel) or the oronasal thermocouple (flow channel) throughout the event identifying it as an apnea. During the first half of the apneic period, there is no evidence of ventilatory effort, but then increasing evidence of effort in the thorax channel is seen leading up to the termination of the apneic event. This is an illustration of a mixed apnea, having central features at onset but then demonstrating obstructive features as the event progresses. |
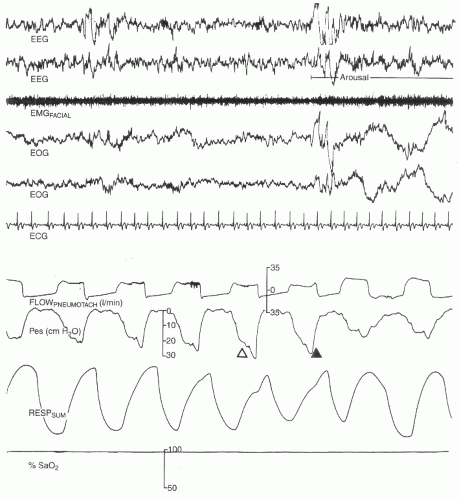 Figure 41.13 Polysomnographic recording showing an example of upper airway resistance syndrome. Note that peak increase in effort (indicated by the solid arrowhead) is associated with a small drop in peak flow and tidal volume, triggering a transient electroencephalographic arousal. ECG, electrocardiogram; EMGFACIAL, facial muscle electromyogram; EOG, electro-oculogram (right and left); FLOWPNEUMOTACH, pnuemotachometer to quantify airflow; Pes, esophageal manometry to record esophageal pressure; RESPSUM, respiratory effort; SaO2, saturation with oxygen. (Reproduced from Chokroverty S. Sleep Disorders Medicine: Basic Science, Technical Considerations and Clinical Aspects. 3rd ed. Philadelphia: Saunders/Elsevier; 2009, with permission.) |
The recurring high-amplitude EEG activity (phase A of the period)
The intervening background EEG activity (phase B of the period)
The period or cycle that is the sum of phase A and phase B
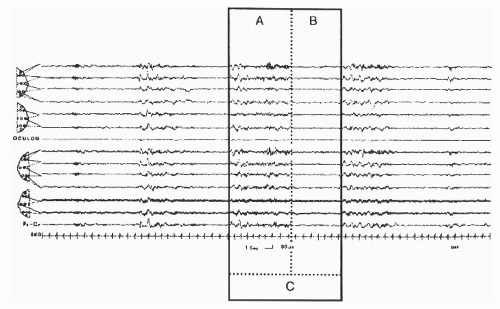 Figure 41.14 An example of CAP in stage N2. The box outlines a CAP cycle (C) composed of phase A and following phase B. Bipolar EEG channels for first six channel top to bottom Fp2-F4, F4-C4, C4-P4, P4-O2, F8-T4, and T4-T6; bottom eight channels are top to bottom Fp1-F3, F3-C3, C3-P3, P3-O2, F7-T3, T3-T5, EOG, and ECG. (From Terzano et al. Atlas, rules, and recording techniques for the scoring of cyclic alternating pattern (CAP) in human sleep. Sleep Med. 2001;2:537-553, with permission.) |
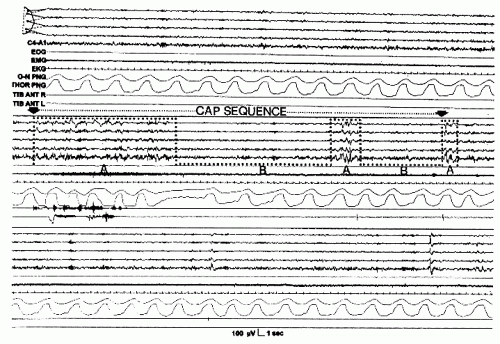 Figure 41.15 Consecutive stretches of non-CAP (top), CAP (middle), and non-CAP (bottom). The middle section illustrates the minimal requirements for definition of a CAP sequence (at least three phase A’s in succession). The CAP sequence occurs between two black arrows and the transition between phases is delineated by the dotted line. EEG derivation is Fp2-F4, F4-C4, C4-P4, P4-O2, and C4-A1. (From Terzano et al. Atlas, rules, and recording techniques for the scoring of cyclic alternating pattern (CAP) in human sleep. Sleep Med. 2001;2:537-553, with permission.) |
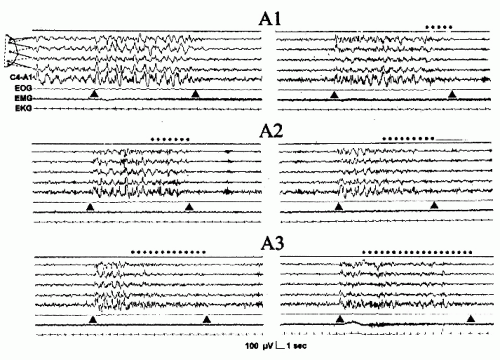 Figure 41.16 The three phase A subtypes. The dotted line indicates the fast low-amplitude portion of phase A. EEG derivation as in Figure 41.15. (From Terzano et al. Atlas, rules, and recording techniques for the scoring of cyclic alternating pattern (CAP) in human sleep. Sleep Med. 2001; 2:537-553, with permission.) |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


