Fig. 5.1
(a) Variable phenotypes of NF2 with bilateral schwannomas with brainstem compression. (b) Auditory function in NF2. At presentation to the neurosurgeon
In those ears observed for some time, possibly because of residual hearing function, by “natural course”, deafness developed on average at the age of 29 years.
5.4 Special Considerations of Preservation of Auditory Nerve Function in NF2 VS
In view of the tremendous difficulty and the tremendous need to preserve at least unilateral hearing in NF2, Samii decided and tried in selected cases to achieve hearing preservation by subtotal tumour resection. The microsurgical principles are as follows:
In the semi-sitting position after retrosigmoid suboccipital craniotomy, CSF is drained from the basal cistern and light cerebellar retraction is carried out. The tumour in the cistern is at first not touched, but the internal auditory canal is drilled open under meticulous monitoring with repeated breaks. The intrameatal tumour is enucleated and is mobilized away from the nerves. In serious ABR deterioration, intrameatal dissection is stopped, ABR recovery is awaited and extrameatal tumour enucleation is performed. In most cases, the extrameatal tumour part will be largely or completely removed while the dissection close to the porus and at the intrameatal portion may be critical. As long as ABR show fast recovery at short breaks of the microsurgical activity, further dissection may be tried; if recovery shows to be slower or incomplete, then the tumour resection should be stopped in order to conserve hearing.
Hearing could be preserved in 29% of NF2 patients (Table5.1). In a series of 23 patients the technique of subtotal resection was applied with successful hearing conservation in 15 cases (65%) (Table 5.2). In critical cases with repeteated ABR deterioration and recovery the administration of vasoactive substances may be beneficial [31].
Table 5.1
Auditory function in 195 tumour operations in 145 neurofibromatosis type 2 patients
Auditory function | Preoperative | Postoperative | |
|---|---|---|---|
H1 (0–20 dB, 100–95 % SDS) | 54 | 8 | |
H2 (21–40 dB, 90–70 % SDS) | 26 | 13 | 36 (29 %) |
H3 (41–60 dB, 65–35 % SDS) | 24 | 7 | |
H4 (61–80 dB, 30–10 % SDS) | 22 | 8 | |
H5 (>80 dB) | 69 | 159 |
Table 5.2
Bilateral vestibular schwannomas. Auditory function in 23 incomplete resections
Case no. | Year of surgery | Size (mm) | Preoperative HL (dB) | SDS (%) | Post-operative HL (dB) | SDS (%) |
|---|---|---|---|---|---|---|
1 | 1986 | 30 × 20 | 1 | 100 | 35 | 90 |
2 | 1987 | 35 × 25 | 2 | 100 | 50 | 70 |
3 | 1989 | 30 × 20 | 30 | 80 | 33 | 80 |
4 | 1990 | 25 × 20 | 5 | 100 | 60 | 70 |
5 | 1990 | 40 × 40 | 43 | 80 | 28 | 90 |
6 | 1991 | 25 × 20 | 6 | 100 | 18 | 100 |
7 | 1991 | 35 × 20 | 7 | 100 | – | – |
8 | 1992 | 35 × 20 | 6 | 95 | – | – |
9 | 1992 | 30 × 20 | 3 | 100 | – | – |
10 | 1993 | 15 × 10 | 10 | 100 | 25 | 90 |
11 | 1993 | 20 × 15 | 7 | 100 | 72 | 35 |
12 | 1993 | 20 × 20 | 1 | 100 | 22 | 100 |
13 | 1993 | 40 × 30 | 32 | 90 | – | – |
14 | 1993 | 20 × 18 | 27 | 90 | 45 | 80 |
15 | 1994 | 10 × 5 | 1 | 85 | 25 | 80 |
16 | 1994 | 15 × 15 | 1 | 100 | 36 | 100 |
17 | 1994 | 20 × 10 | 7 | 90 | 11 | 90 |
18 | 1994 | 50 × 40 | 55 | 60 | – | – |
19 | 1995 | 20 × 15 | 40 | 65 | 46 | 50 |
20 | 1997 | 15 × 13 | 20 | 100 | – | – |
21 | 1997 | 20 × 12 | 15 | 90 | – | – |
22 | 1997 | 7 × 5 | 6 | 100 | 11 | 100 |
23 | 1998 | 28 × 25 | 46 | 100 | – | – |
This method requires detailed patient information and counselling beforehand. In patients in whom auditory function is of great importance, early surgery at good starting conditions must be recommended; in case of a tumorous nerve change or very sensitive ABR, the subtotal technique with bony decompression of the cranial nerves increases the chances of functional preservation.
Long-term follow-up showed that these patients kept some useful function for several years, in general over 10 years and single cases over 14 years. Function remains useful also in case of tumour regrowth for a long time, thanks to the decompression of the internal auditory canal.
However, vestibular schwannomas in NF2 show recurrence usually after four to eight years and cause, among other problems, secondary deafness on previously preserved functional ears. Other patients become deaf early on during their illness. Many of these patients are interested to receive an auditory implant, a cochlea implant or an auditory brainstem implant.
5.5 Cochlea Implant in NF2
A few conditions predispose patients to have successful cochlea implant therapy. NF2 patients with rather small tumours and sudden complete hearing loss are likely to have a failure of their cochlea function. Furthermore, patients with serious amplitude decrease of component I and of the electrocochleography potential during surgery may have cochlea failure, but a still functioning auditory nerve. By promontory stimulation test, positive cochlear nerve function can be identified and the option for a cochlea implant can be formulated.
By a CI, the patient may regain very useful auditory function [10]; however, if tumour is still present and especially if it is infiltrative, CI function will deteriorate over time. If the tumour is a meningioma, the quality and stability of CI function might be superior to the schwannoma situation, even in a relatively large tumour.
The general rule that CI function is always superior to brainstem implant function holds not true for all NF2 patients.
5.6 Auditory Brainstem Implants (ABI) in NF2
Auditory brainstem implants make use of the same technology as cochlea implants, but they contain a different kind of electrode and are designed to be laid onto the cochlear nucleus of the brainstem surface. The very first ABI models contained only two electrodes and were applied by Hitselberger and colleagues [9] at the House Ear Institute in 1979 [1, 4, 9]. Several companies producing ABI have developed different shapes with platinum iridium platelet-shaped electrodes in a silicone carrier. Two models have been used first, the Nucleus Device which contains a magnet, which can be removed temporarily under local anaesthesia to perform an MRI (Fig. 5.2a) [21] or the magnet-free Clarion Device (Fig. 5.2b) and more recently the Medel ABI which contains a non-removable magnet and which is compatible with 1.5 Tesla MRI (Fig. 5.2c) [11].
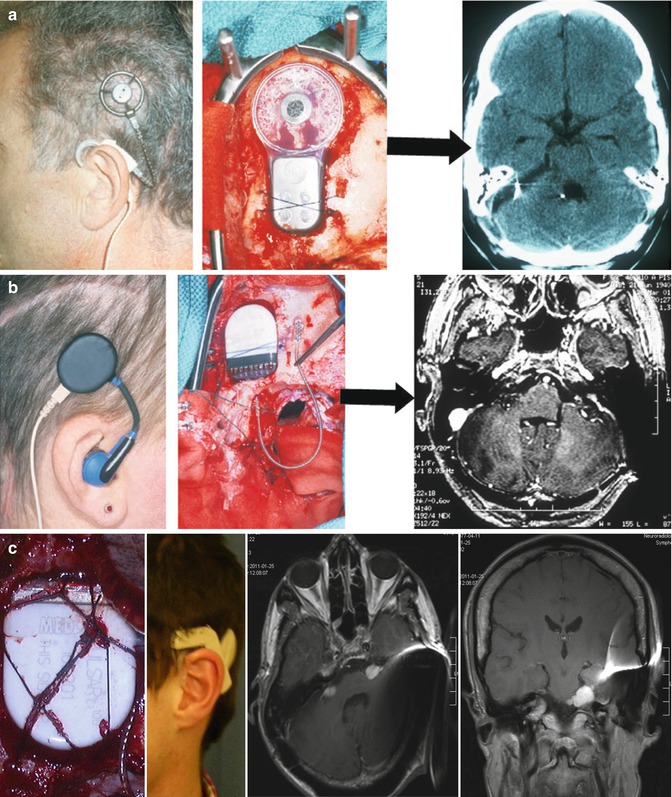
Fig. 5.2
(a, b) Auditory brainstem implant (ABI) models. (a) ABI with removable magnet. (b) ABI without a magnet. (c) This ABI contains a non-removable magnet, officially authorized for magnetic resonance imaging. The magnet causes some image distortion, but analysis of the regions of interest is still possible. If an area is obscured on transverse slices, coronal slices do outline the lesion sufficiently
5.7 Preconditions to ABI in NF2
If the patient has a personal interest in hearing and understanding and undertakes efforts in lipreading, these are favourable factors with regard to the chances of relearning some hearing [28]. Besides, it is sensible to plan the ABI surgery at a rather stable period of the NF2 disease, whereas it is disadvantageous to decide on it when there is multiple tumour progression and a necessity to several operations anyway.
The individual risks have to be analysed and weighed against the possible chances and usefulness. Some patients are by far more affected by spinal cord compression and impending paraparesis or by multiple caudal cranial nerve palsies.
A further specific indication to ABI may be impending visual loss. Most NF2 patients have long-standing visual deficits due to retinal disease and may use only one eye for communication and reading. If that eye is endangered by skull base or intraorbital tumour, in most cases meningioma, then ABI should be implanted early on to enable hearing learning along with some lipreading as long as it is still possible.
Related posts:
 Preoperative Visualization of the Facial Nerve Using Diffusion Tensor Imaging Fibre Tracking in Patients with Large Vestibular Schwannomas
Considerations for Experimental Neuromodulation Following Grafting of the Spinal Cord to Skeletal Muscles for Clinical Application
Chordomas and Chondrosarcomas
Preservation of the Olfactory Tract in Bifrontal Craniotomy
The Surgical Management of Trigeminal Schwannomas
Bypass and Vascular Reconstruction for Posterior Circulation Aneurysms
Preoperative Visualization of the Facial Nerve Using Diffusion Tensor Imaging Fibre Tracking in Patients with Large Vestibular Schwannomas
Considerations for Experimental Neuromodulation Following Grafting of the Spinal Cord to Skeletal Muscles for Clinical Application
Chordomas and Chondrosarcomas
Preservation of the Olfactory Tract in Bifrontal Craniotomy
The Surgical Management of Trigeminal Schwannomas
Bypass and Vascular Reconstruction for Posterior Circulation Aneurysms
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


