Chapter 14 Radiofrequency Rhizotomy for Facet Syndrome
 At the cervical level, the facet joint appears to be an important source of pain with degenerative neck symptoms. More than 50% of patients presenting to a pain clinic with neck pain may have facet joint–related pain.
At the cervical level, the facet joint appears to be an important source of pain with degenerative neck symptoms. More than 50% of patients presenting to a pain clinic with neck pain may have facet joint–related pain.








 In the group of patients attending a pain clinic for neck pain, facet joints are probably involved in more than 50% of cases.
In the group of patients attending a pain clinic for neck pain, facet joints are probably involved in more than 50% of cases.

 Lumbar paravertebral tenderness is suggestive of pain originating from the zygapophyseal (facet) joints.
Lumbar paravertebral tenderness is suggestive of pain originating from the zygapophyseal (facet) joints.



 Although radiological examinations may point out degenerative zygapophyseal (facet) joints, no correlation is established between radiological abnormalities and pain originating from these joints.
Although radiological examinations may point out degenerative zygapophyseal (facet) joints, no correlation is established between radiological abnormalities and pain originating from these joints.
Cervical Facet Pain
Establishing the Diagnosis
Background
Neck pain is defined as pain in the area between the base of the skull and the first thoracic vertebra. Pain extending into adjacent regions is defined as radiating neck pain. Pain may radiate into the head (cervicogenic headache), shoulder, or upper arm (radicular or nonradicular pain).1 A distinction is made between trauma-related neck pain (whiplash-associated disorders) and degenerative neck problems. Because the causes of neck pain often are unclear, a distinction is made between the cause and source.2 The following innervated structures in the neck may be sources of pain: vertebrae, discs, uncovertebral (Luschka) joints, ligaments, muscles, and facet (zygapophyseal) joints.
Cervical facet syndrome is defined as a combination of symptoms:




There is a great deal of research into degenerative signs of the cervical vertebral column. In the discus intervertebralis (1) annular tears, (2) discus intervertebralis prolapse, and (3) endplate damage and internal discus intervertebralis disruption have been identified as potential structural discus intervertebralis pathologies.3 Other structures in the neck, such as the facet joints and uncovertebral joints, may also show degenerative signs. The hypothesis that discus intervertebralis degeneration and discus intervertebralis narrowing increase facet joint loading and consequently facet osteoarthritis seems plausible but has yet to be proven. Some researchers claim that the discus intervertebralis and the facet joints can be seen as independent pain generators.4
Compared with research on lumbar facet pain, research on cervical facet dysfunction is relatively recent. In 1988, Bogduk and Marsland5 described the positive effect of injection of local anesthetics close to the facet joints in patients with neck pain. Dwyer et al6 showed that injection of irritating substances into the facet joints results in a specific radiation pattern (Fig. 14-1). The same radiation pattern is seen with mechanical and electrical stimulation. However, because it was later demonstrated that stimulation of the discus intervertebralis produces the same radiation pattern as stimulation of the facet joints, this is probably a segmental phenomenon.
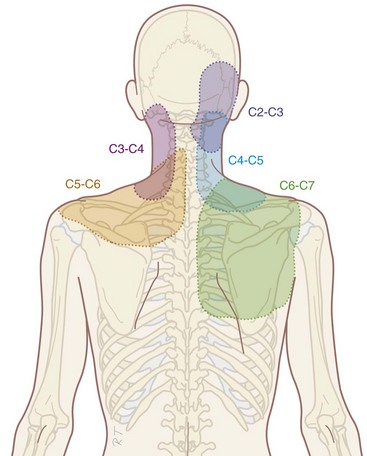
Fig. 14-1 Radiation pattern of cervical facet pain.
(Illustrated by Rogier Trompert Medical Art. http://www.medical-art.nl.)
Physical Examination
Flexion and extension: passive and active
Lateroflexion: passive and active
Rotation in maximal flexion: passive and active
Local pressure pain over the facet joints can indicate problems arising from the facet joints. Recent research showed that local pressure, defined as pain with pressure of at least 4 kg, is a predictor of success of RF treatment (see Radiofrequency Treament sections).7 When the neck pain is accompanied by radiation to the shoulder region, shoulder pathology should be excluded.
There is no evidence for the relation between the results of clinical examination and the history with the presence of pain originating from the cervical facet joints.8 In daily clinical practice, history and physical examination are useful to exclude serious pathology and to obtain a working diagnosis. An indication of the segmental level (high, mid, or low cervical) involved can be obtained.
Diagnostic Blocks
The working diagnosis of facet pain based on history and clinical examination may be confirmed by performing a diagnostic block. Local anesthetic can be injected intraarticularly or adjacent to the ramus medialis (medial branch) of the ramus dorsalis of the segmental nerve.2,9 Diagnostic medial branch block procedures are performed under fluoroscopy. There is no consensus about the definition of a successful diagnostic block. Some authors claim that 100% pain relief should be achieved.10 But Cohen et al7 showed that there is no difference in outcome of the RF treatment of patients reporting 80% and those reporting more than 50% pain reduction after a diagnostic block. In daily clinical practice, we consider a diagnostic block successful if more than 50% pain reduction is reported.
To minimize the number of false-positive results, a number of researchers have suggested that a second block should be carried out using a local anesthetic with different duration of action (e.g., lidocaine and bupivacaine; comparative double blocks). Only if the patient responds concordantly (longer or shorter pain reduction depending on the duration of action of the local anesthetic) is this indicative of facet joint pain. This is not an etiological but a pharmacological criterion. These researchers suggest that double blocks are the gold standard for the diagnosis of facet pain. A gold standard, however, should be generally accepted and used. The concept of double blocks has theoretical and practical shortcomings. A best evidence synthesis on the assessment of neck pain concluded that diagnostic facet injections have not been validated to identify facet joint pain.11
In summary, on the basis of history and physical examination, a working diagnosis of cervical facet pain is defined. One diagnostic block can be recommended for confirming the clinical working diagnosis of facet pain. A block is considered positive when the patient experiences 50% pain reduction.7
Differential Diagnosis
Chronic pain diagnoses such as segmental dysfunction, instability, and muscle strain are not sufficiently documented to be included in the differential diagnosis.2 A summary of the differential diagnosis is represented in Table 14-1.
Table 14-1 Differential Diagnosis in Axial Neck Pain without Irradiation
| Tumors | |
| Infections | Discitis, septic arthritis, osteomyelitis, meningitis, epidural abscess |
| Trauma | Fractures, whiplash-associated disorders |
| Rheumatoid arthritis | |
| Crystal arthropathies | e.g., Gout |
| Vascular disorders | Aneurysm |
| Neurological causes* | Neuromas |
| Degenerative disorders | Spondylosis, osteoarthrosis |
* Neurological causes are almost always accompanied with loss of neurological function.
Anatomy
The cervical facet joint capsules are longer and looser than the facet joint capsules in the thoracic and lumbar regions.12 The more or less flat facet joint surfaces from C2 to C7 form an angle of approximately 45 degrees with the longitudinal axis through the cervical spinal column with a large range of intra- and interindividual variability. Compared with the lumbar facet joints, the cervical facet joints have a high density of mechanoreceptors. McLain took twenty-one cervical facet joint capsules and surrounding tissue from three human subjects by block-excision and processed them in a modified gold chloride technique.13 In twenty-five micron serial histological sections he identified, according to the classification of Freeman and Wyke, encapsulated Type I, II, and III mechanoreceptors and non-encapsulated Type IV mechanoreceptors. The Type II receptors were found most frequently, mainly localized in the dens, fibrous joint capsule. Fewer Type I receptors were identified in both the capsule and the areolar, loose connective tissue. Only a handful of Type III receptors were found, at the junction between the capsule and the loose connective, sub-synovial tissue. Unencapsulated, nociceptive Type IV free nerve endings were present throughout the capsule, synovium, and areolar tissue.14
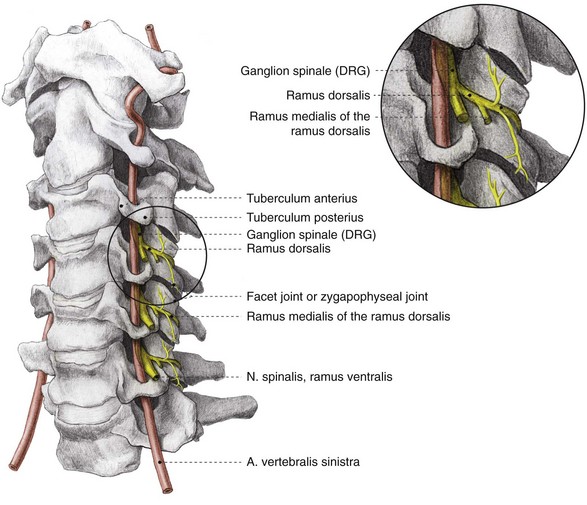
The facet joints from C3 to C7 are innervated by the ramus medialis (medial branch) of the ramus dorsalis of the segmental nerve (Fig. 14-2). Each facet joint is innervated by nerve branches from the upper and lower segments (Fig. 14-3).15

Imaging
In specific cases, plain radiography of the cervical spinal column (two or three directions) can be indicated to exclude tumor or fracture. Plain radiography does not, however, provide information for establishing the diagnosis of facet problems. This examination can help in estimating the degree of degeneration. The anterior spinal column is inspected for narrowing of the discus intervertebralis and anterior and posterior osteophyte formation. The posterior spinal column is inspected for facet osteoarthritis (facet sclerosis and osteophyte formation). In 1963, Kellgren et al16 stated that when degenerative changes are seen on plain radiography, anatomical degeneration has already reached an advanced stage.
With progressing age, degenerative changes are more frequently seen: 25% at the age of 50 years up to 75% at the age of 70 years.17 An age-related prevalence study concerning facet joint involvement in chronic neck pain indicates a comparable prevalence among all age groups.18
Degenerative changes of the cervical spinal column are present in asymptomatic patients, indicating that degenerative changes do not always cause pain. However, the conclusion that there is no relation between degeneration and pain cannot be drawn. There are studies indicating a relationship between degenerative changes and pain symptoms.17,19
Guidelines
Recently, the following classification for neck pain and associated symptoms has been proposed:20
 Grade I neck pain: No symptoms indicating serious pathology and minimal influence on daily activities
Grade I neck pain: No symptoms indicating serious pathology and minimal influence on daily activities


The following interventions are published options for the treatment of cervical joint pain:



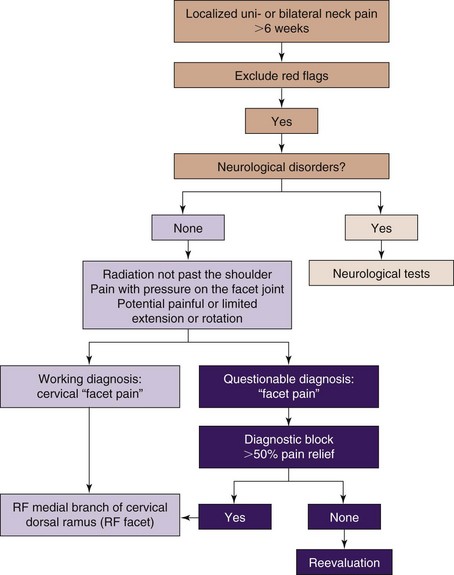
A practice algorithm for the management of facet pain is illustrated in Fig. 14-4.
Indications and Contraindications
Chronic neck pain can be caused by the facet joints. Percentages between 25% and 65% are described, depending on the patient group and selection method. In the group of patients attending a pain clinic for neck pain, it is likely to be more than 50%.21,22 Conservative treatment options for cervical facet pain such as physiotherapy, manipulation, mobilization, and pharmacological treatment are frequently applied before considering interventional treatments.
Corticosteroid injections are performed after a careful risk-to-benefit analysis in patients with metabolic diseases such as diabetes. Psychological factors such as avoidance behavior and catastrophizing are less commonly related to neck symptoms in contrast to patients with low back problems.2
Technique
Percutaneous Facet Denervation
The (postero-)lateral approach in the supine position is described below (Fig. 14-5). The advantage of this technique is that it is possible to maintain eye contact with the patient. Sedation is rarely required.
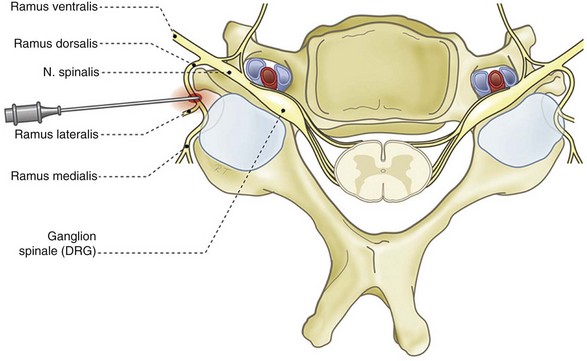
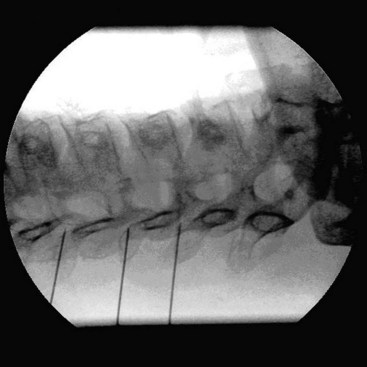
The patient is placed in the supine position with the head slightly extended on a small cushion. The C-arm is placed in an oblique position (±30 degrees). In this position, the beam runs parallel with the exiting nerve root that runs somewhat caudofrontal. Also in this position, the pedicles from the contralateral side are projected on the anterior half of the vertebral body. In the frontal plane (anteroposterior [AP] direction), the C-arm is positioned in a small angle with respect to the transverse plane. In this position, the discus intervertebralis space and neuroforamen are visible (Fig. 14-6). The ramus medialis (medial branch) of the ramus dorsalis runs over the base of the processus articularis superior. The injection point is marked on the skin, slightly posterior and caudal to the end point of the needle that is dorsal to the posterior boundary of the facet column. The first needle is introduced in a horizontal plane, slightly cranially so the tip of the needle points in the direction of the end point. It is important to understand that this is not a “tunnel-view” technique. The needle is slowly advanced anteriorly and cranially until bony contact with the facet column occurs. The farther the needle is advanced, the more difficult it becomes to change the direction. Therefore, the position of the needle needs to be checked frequently. If the needle points too much in the direction of the neuroforamen without contacting bone, the direction needs to be corrected to be more posterior. If there is no bone contact in the posterior direction, there is a risk that the needle will enter the spinal canal between the laminae. To prevent this, the needle position can be checked in the AP direction. The final position of the needle in the AP direction is in the concave “waist” of the facet column. After placement of the first needle, the other needles are introduced in the same way. The first needle acts as a guide to direction and depth.
The same technique is used for the facet joints of C3-C4 to C6-C7. For the facet joint of C2-C3, a different end point for the needle is used, just beneath the C2-C3 joint.23
Outcomes Evidence
The recently published Evidence-Based Practice Guidelines based on clinical diagnoses based the recommendations on the “grading strength of recommendations and quality of evidence in clinical guidelines” described by Guyatt et al24 and adapted by van Kleef et al25 in an editorial in Pain Practice (Table 14-2).
Table 14-2 Summary of Evidence Scores and Implications for Recommendation
| Score | Description | Implication |
|---|---|---|
| 1A+ | Effectiveness demonstrated in various RCTs of good quality. The benefits clearly outweigh the risks and burdens. | } Positive recommendation |
| 1B+ | One RCT or more RCTs with methodological weaknesses demonstrate effectiveness. The benefits clearly outweigh the risks and burdens. | |
| 2B+ | One or more RCTs with methodological weaknesses demonstrate effectiveness. The benefits are closely balanced with the risks and burdens. | |
| 2B± | Multiple RCTs, with methodological weaknesses, yield contradictory results better or worse than the control treatment. The benefits are closely balanced with the risks and burdens or there is uncertainty in the estimates of benefits, risks, and burdens. | } Considered, preferably study related |
| 2C+ | Effectiveness is only demonstrated in observational studies. Given that there is no conclusive evidence of the effect, benefits are closely balanced with the risks and burdens. | |
| 0 | There is no literature or there are case reports available, but these are insufficient to prove effectiveness or safety. These treatments should only be applied in relation to studies. | Only study related |
| 2C− | Observational studies indicate no or too short-lived effectiveness. Given that there is no positive clinical effect, the risks and burdens outweigh the benefits. | } Negative recommendation |
| 2B− | One or more RCTs with methodological weaknesses or large observational studies that do not indicate any superiority to the control treatment. Given that there is no positive clinical effect, the risks and burdens outweigh the benefits. | |
| 2A− | RCT of a good quality that does not exhibit any clinical effect. Given that there is no positive clinical effect, the risks and burdens outweigh the benefits. |
RCT, randomized controlled trial.
Related posts:
 Facet (Zygapophyseal) Intraarticular Joint Injections
Facet (Zygapophyseal) Intraarticular Joint Injections
 Fluoroscopy, Ultrasonography, Computed Tomography, and Radiation Safety
Fluoroscopy, Ultrasonography, Computed Tomography, and Radiation Safety
 Nerve Destruction for the Alleviation of Visceral Pain
Nerve Destruction for the Alleviation of Visceral Pain
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


