Chapter 15 Sacroiliac Joint Injections and Lateral Branch Blocks, Including Water-Cooled Neurotomy
 Pain attributable to SIJ dysfunction is an area approximately 3 × 10 cm just inferior to the posterior superior iliac spine and usually not superior to L5.
Pain attributable to SIJ dysfunction is an area approximately 3 × 10 cm just inferior to the posterior superior iliac spine and usually not superior to L5.



 Exclude other etiologies (e.g., lumbar facet joint arthropathy, hip joint arthropathy) as pain generators.
Exclude other etiologies (e.g., lumbar facet joint arthropathy, hip joint arthropathy) as pain generators.




Establishing a Diagnosis
Goldthwaite and Osgood, in 1905, first described “sacroiliac strain” as a possible source of low back pain1 and the sacroiliac joint (SIJ) was considered the primary source of low back pain in the early 20th century.2 In 1936, Pitkin and Pheasant described lower extremity pain as originating in the sacroiliac and lumbosacral joints and their accessory ligaments and coined the term sacroarthrogenic telalgia. SIJ fusion became the treatment of choice for radicular pain originating from the low back.3 It was not until Mixter and Barr that focus was placed on the lumbar spine, the intervertebral disc, and the herniation of nucleus pulposus contents.4 Today, there is a reemergence implicating the SIJ as a potential source of low back pain with an estimated prevalence among patients with low back pain of 18% to 30%.5,6
Pathology of the SIJ has been documented in a variety of conditions; structural abnormalities, joint infections, metabolic and inflammatory disorders, and degeneration have all been implicated.7 SIJ dysfunction or SIJ syndrome is a condition in which pain localized to the SIJ cannot otherwise be explained by an identifiable pathological process (e.g., joint infection). Clinically distinguishing primary SIJ dysfunction from the other etiologies that overlap in pain referral patterns may be difficult. Much of the confusion regarding the diagnosis of SIJ dysfunction revolves around the inability to differentiate SIJ pain from pain that originates from surrounding structures. For example, discogenic and facet joint pathology have a clinical presentation similar to that of SI joint pathology. Not only are the pain distributions considered similar in many references, but the clinical tests used in diagnosis (e.g., Patrick’s, Gaenslen’s) are known to stress surrounding structures.7 The familiar symptom in SIJ dysfunction is the pain or other symptoms ascribed to a rectangular area approximately 3 × 10 cm just inferior to the posterior superior iliac spine (PSIS) identified on a pain drawing; however, no clinical studies have demonstrated this as a consistent finding for diagnosing SIJ dysfunction.8 Through patient history and diagnostic testing, several referral patterns have been proposed, although these referral patterns may be present in other sources of low back pain.9
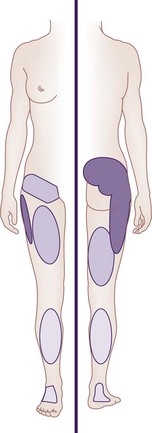
Furthermore, referral of pain into various locations of the lower extremity does not distinguish SIJ pain from other pain states.5,10 However, only 4% of patients with SIJ pain mark any pain above the L5 on self-reported pain drawings.10 The multiple patterns of SIJ pain referral zones may arise for several reasons: SIJ innervation is highly variable and complex; pain may be somatically referred from other primary osseous and ligamentous nociceptors such as the zygapophyseal joint, intervertebral disc, or adjacent structures (e.g., piriformis muscle, sciatic nerve, and L5 nerve root); and the referral pattern may be affected by intrinsic joint pathology and become active nociceptors.1 Slipman et al11 examined pain referral patterns in patients with SIJ dysfunction and reported that 94% of patients had pain radiating into the buttock, lower lumbar region (72%), lower extremity (50%), groin area (14%), upper lumbar region (6%), and abdomen (2%). In 28% of patients, the pain radiated distal to the knee, and 14% described foot pain (Fig. 15-1).
SIJ syndrome may occur acutely from trauma, sudden heavy lifting, prolonged lifting and bending, torsional strain, rising from a stooped position, a fall onto the buttock, or rear-end motor vehicle accident with the ipsilateral foot on the brake.1 Characteristically associated with SIJ dysfunction include buttock pain caudal to the PSIS; pseudoradiculopathy with pain radiating to the posterolateral aspect of the thigh (at times caudal to the knee); and aggravation of pain in sitting position, rising from a sitting position (exiting an automobile), and relieved by changing positions. The most consistent factor for identifying patients with unilateral SIJ pain is unilateral pain localized predominantly below the L5 spinous process.5,7,8,10,12
Physical Examination
In 1994, the International Association for the Study of Pain (IASP) proposed a set of criteria for diagnosing SIJ pain, referring to patients with pain in the area of the SIJ, which should be reproducible by performing specific pain provocation tests or should be completely relieved by infiltration of the symptomatic SIJ with local anesthetics.13 An assortment of SIJ examination maneuvers has been described to diagnose SIJ dysfunction (Box 15-1). Problematic to this is that provocation in this area may incite pain in adjacent structures, confounding the diagnosis of SIJ dysfunction. Additionally, using individual tests (provocative, motion, or palpation) has yielded low sensitivity or specificity for detecting a pathological SIJ.14–16 Dreyfuss et al,10 examining the usefulness of medical history and physical examination, concluded that no historical feature, none of the 12 tested SIJ maneuvers, and no ensemble of these 12 maneuvers demonstrated worthwhile diagnostic value. These results are replicated in a prospective cohort study in which provocative maneuvers were not predictive of diagnosis of SIJ dysfunction.17 Additionally, 20% of asymptomatic patients have been found to possess pain on provocative tests at the SIJ.18 In contrast, other reports indicate the usefulness of a combination of tests that increases the likelihood of response to SIJ injections.19–21 In a study examining the diagnostic validity of tests that could be ascribed to the IASP criteria for diagnosing SIJ pain, tests such as pain mapping or pain referral patterns have an ability to correctly identify patients with SIJ pain. However, they fail in discriminating patients without SIJ pain. The compression and thigh thrust test were regarded as positive examination finding in diagnosing SIJ pain.22 The general consensus appears to be that SIJ pain can be diagnosed with reasonable certainty with controlled comparative local anesthetic diagnostic blocks.23,24
Box 15-1 Sacroiliac Joint Examination Stress Maneuvers
| Patrick (FABERE) test | With the patient supine, the thigh is flexed, and the ankle is placed above the knee of the contralateral leg. The ipsilateral knee is depressed, the contralateral hip is stabilized, and the ankle is maintained in its position above the contralateral knee. A positive test result is indicated by the patient’s complaints of pain over the ipsilateral SIJ as the knee is depressed toward the examination table. |
| Gaenslen’s test | With the patient supine, the ipsilateral leg hangs over the examination table and the contralateral leg is flexed, bringing the knee towards the abdomen. Counterpressure is applied to the knee of the hanging leg, toward the floor, and the contralateral leg toward the abdomen. A positive test result is indicated by the patient’s complaints of pain over the ipsilateral SIJ as counterpressure is applied. |
| Fortin’s finger test (sacral sulcus tenderness) | The patient is asked to point to the region of pain with one finger. A positive test result is indicated by consistent localization of pain in an area immediately inferomedial to the PSIS within 1 cm. |
| Shear test | With the patient prone, pressure is applied in a caudal direction. A positive test result is indicated by the patient’s complaints of pain over the SIJ as pressure is applied. |
| Compression test | With the patient in lateral decubitus position, the hips and knees are flexed. Downward force is applied to the uppermost iliac crest. A positive test result is indicated by the patient’s complaints of pain over the SIJ as pressure is applied. |
| Gillet test | With the patient standing, the PSIS is palpated along with the sacral spinous processes. The patient flexes the ipsilateral hip and knee to a minimum of 90 degrees. A positive test result is indicated by the thumb on the PSIS moving cephalad in relation to the thumb on the sacrum. |
| Yeoman’s test | With the patient prone, the hip is extended, and the ipsilateral ilium is rotated. A positive test result is indicated by the patient’s complaints of pain over the SIJ as pressure is applied. |
PSIS, posterior superior iliac spine; SIJ, sacroiliac joint.
Anatomy
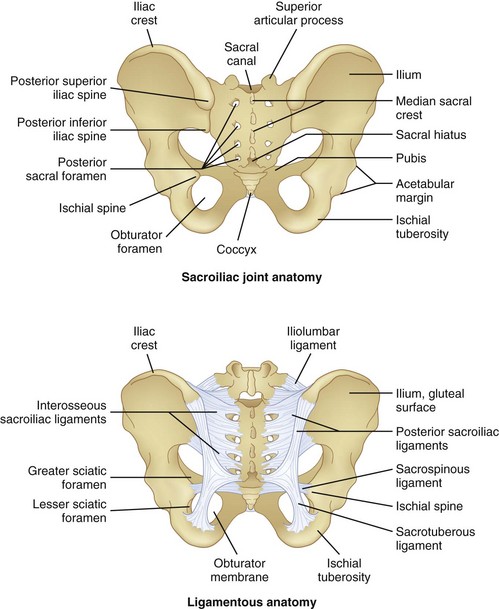
The SIJ is the largest axial joint in the body, with an average surface area of 14 to 17.5 cm2.25,26 It is a diarthrodial joint, with the anterior third being synovial and the remaining posterior aspect a syndesmosis, composed of interosseous ligament connections (Fig. 15-2). An auricular-shaped joint oriented in an oblique medial to lateral direction, morphological variability exists in the adult SIJ with respect to size, shape, and surface contour.27 The posterior aspect of the joint has a fibrous capsule but may lack synovial continuity with the anterior aspect of the joint. Designed for stability, the SIJ is a triplanar shock absorber, transmitting and dissipating upper trunk loads to the pelvis, force from the lower extremities during ambulation, and facilitates parturition. The SIJ rotates about all three axes, although the predominant motion appears to be x-axis rotation with some z-axis translation.1 Motion of the SIJ is usually limited to 1 to 3 degrees of rotation and 1.6 mm of translation, with 90 percent of rotation occurring along the x-axis.1 The SIJ motion progressively decreases, and motion at the joint may become markedly restricted secondary to increased cartilage; reduced density of chondrocytes, causing deep fissures in the cartilage; and fibrous connections among the auricular facets.28 As the capsule becomes increasingly collagenous and fibrous, ankylosis occurs, and by the eighth decade of life, erosions and plaque formation are inevitable and ubiquitous.29
Innervation
Variability and lack of precise innervation of the SIJ remains, but it has been suggested that the ventral side of the SIJ is usually supplied by L4 through S2 spinal nerves, the caudal side by the superior gluteal nerve, and the dorsal side by S1 and S2 spinal nerves.30 Others have implicated the ventral rami of L4 and L5, the superior gluteal nerve, and the dorsal rami of L5, S1, and S2.31 Some authors have even suggested that the anterior SIJ is devoid of nervous tissue32 and that the posterior SIJ is supplied by L3 and S4.33 Additionally implicated are the L5 dorsal ramus and the lateral branches of the S1-S3,34 and this description is the focus of ablative therapy in the attenuation of SIJ pain.
Basic Science
Intraarticular structures possess nerve fibers, which are sensitive for pain and support the theory that nociceptive signals may originate from the intraarticular structures of the SIJ.35 Additionally, as previously described, innervation exists for the SIJ, and the intraarticular nociceptive fibers and the lumbosacral innervation are intended for interventions. There is not a “gold standard” for the diagnosis of SIJ dysfunction, but the rationale for the use of SIJ blocks as standard for diagnosing SIJ pain is based on the fact that SIJs are richly innervated and have been shown to be capable of being a source of low back pain and referred pain in the lower extremity.36
Therapeutic interventions in the treatment of SIJ pain include manual manipulation, prolotherapy, intraarticular injections, ablative procedures, and surgical interventions. Minimally invasive procedures, including intraarticular injections and ablative procedures, are minimally destructive to anatomy. Serial intraarticular injections of local anesthetics and steroids are thought to reduce the inflammatory response and the resultant joint symptomatology. Multiple studies have evaluated the effectiveness of intraarticular injections and ablative procedures (see Outcomes Evidence). Ablative procedures have included conventional radiofrequency (RF), pulsed RF (PRF) denervation, and cooled RF denervation of the SIJ. Conventional RF37 and PRF38 of the lateral branches have been reviewed and discussed by others.
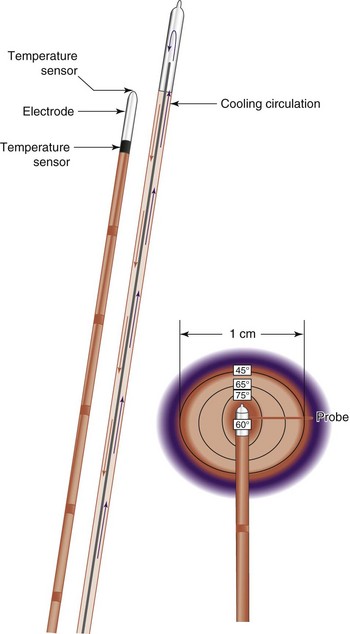
The inherent challenge when treating patients with SIJ pain with RF energy is the inconsistent location of targeted lateral branch nerves.39,40 The lateral branches supplying afferent information from pain-generating SIJs form a complex arcade of small nerve fibers anastomosing with multiple dorsal rami at each foramen. The location of these branches is unpredictable, varying from patient to patient, side to side, and level to level.39 Additionally, conventional RF tissue ablation efficacy is limited by the lesion size secondary to impedance created by tissue desiccation, tissue boiling, and carbonization around the electrode tip. Carbonization is probably the most important cause of the increased impedance and leads to an abrupt decrease in lesion current (and delivered power), such that no more energy is delivered around the electrode and no additional tissue heating occurs.41 Cooled RF energy generates heat in the surrounding tissue, and internal cooling of the electrode moderates temperature near the tip (Fig. 15-3). Internal cooling enhances lesion size by removing the constraint of high-temperature charring in tissue adjacent to the electrode, thus allowing effective ionic heating at a greater distance.42
Related posts:
 Facet (Zygapophyseal) Intraarticular Joint Injections
Facet (Zygapophyseal) Intraarticular Joint Injections
 Fluoroscopy, Ultrasonography, Computed Tomography, and Radiation Safety
Fluoroscopy, Ultrasonography, Computed Tomography, and Radiation Safety
 Nerve Destruction for the Alleviation of Visceral Pain
Nerve Destruction for the Alleviation of Visceral Pain
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


