Sleep and sleep disorders are frequently overlooked as a cause or exacerbating factor in neurologic dysfunction. Neuronal activity and the networks involved are different in each state of sleep (nonrapid eye movement [NREM] and rapid eye movement [REM] sleep) compared with the normal waking brain. Sleep and sleep disorders therefore offer unique opportunities to understand the physiology of the brain and its impact on daily functioning. Sleep is involved in the regulation of endocrine and autonomic output and is integral to learning and memory, areas whose complexity and relationship to sleep are only beginning to be understood.
This chapter begins with a brief description of normal sleep and its impact on functioning. Diagnostic testing in sleep is discussed in Chapter 29. An overview of sleep disorders follows with particular relation to their impact on neurologic diseases.
PHYSIOLOGY OF NORMAL SLEEP
Sleep is an active process that involves numerous distinct neuronal networks, which are ultimately expressed as altered physiologic functions. Heart rate, blood pressure, gas exchange, gastrointestinal function, hormonal secretion, and even kidney function are altered during sleep. The exact purpose of sleep remains unclear, but there is considerable evidence of essential associations with immune function, memory, learning, energy conservation, and toxin clearance.
Sleep is classified into stages based on three parameters: electroencephalography (EEG), eye movement or electro-oculography (EOG), and muscle tone as assessed by electromyography (EMG) of the mentalis muscle. Arbitrary classification of 30 second recordings, or epochs, divide the process into wakefulness, three stages of NREM sleep (stages N1, N2, and N3), and one stage of REM sleep (stage R).
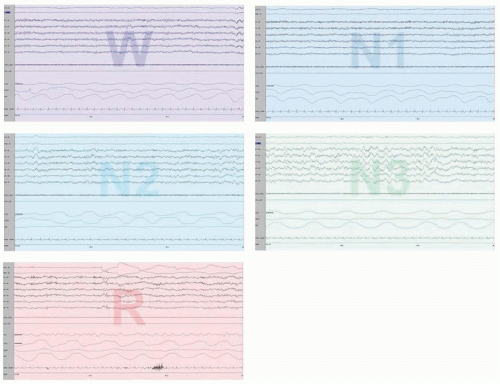
Wakefulness (stage W) is identified by a low-voltage fastfrequency EEG, high muscle tone, and REMs. Stage N1 sleep is characterized by a low-voltage, mixed-frequency EEG and slow, rolling eye movements. Reactivity to outside stimuli is decreased, and mentation may proceed but is slowed. Stage N2 consists of a moderate low-voltage background EEG with sleep spindles (bursts of 12- to 16-Hz activity lasting 0.5 to 2 seconds) and K complexes (brief high-voltage discharges with an initial negative deflection followed by a positive component). Slow-wave sleep (stage N3) consists of high-amplitude delta (0 to 2 Hz) frequencies occupying 20% or more of the epoch. During this deeper sleep, heart and respiratory rates are slowed and regular. In NREM sleep, the tonic chin EMG is of moderately high amplitude but less than that of quiet wakefulness (Fig. 114.1).
The EEG pattern during REM sleep (stage R) consists of lowvoltage, mixed-frequency activity and is similar to that of stage N1 sleep. Moderately high-amplitude, 3- to 6-Hz triangular waveforms referred to as sawtooth waves are intermittently present and are unique to REM sleep. Intermittent bursts of rapid conjugate eye movements occur. Tonic chin EMG activity is absent or markedly reduced, and phasic muscle discharges occur in irregular bursts. The decreased EMG activity is a reflection of muscle paralysis resulting from active inhibition of muscle activity. During REM sleep, surges of parasympathetic and sympathetic activity are denoted by greater variability in heart and respiratory rates. This stage is also associated with complex vivid imagery, but visual imagery can occur in all sleep stages. When occurring in deep NREM sleep, dream images are typically fragmented and may be associated with actions such as the sensation of falling.
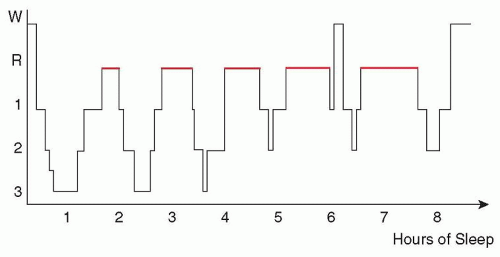
During a normal night, sleep comprises recurring cycles. Within each cycle of 90 to 120 minutes, NREM sleep alternates with REM sleep. The normal healthy adult typically falls asleep within 10 minutes and goes through the sequence of stages N1 through N3, followed by reversion to stage N2 sleep. Afterward, the first REM sleep period occurs 70 to 100 minutes into sleep. The first REM period is usually the shortest, about 10 minutes. This pattern of NREM and REM sleep is repeated three to five times during a normal night’s sleep. Typically, most stage N3 sleep is seen in the first two sleep cycles, and REM sleep periods increase in duration and intensity of REM activity as the night progresses. Stage N2 sleep, however, is the most common sleep stage, typically making up half of a normal adult’s night. In the normal adult, wakefulness accounts for approximately 5% of the night. N3 and REM sleep typically account for 25% each of total sleep and N1 approximately 5% (Fig. 114.2).
NEUROANATOMY AND NEUROCHEMISTRY OF SLEEP
Anatomically, NREM sleep is expressed when a network of neurons in the anterior hypothalamus suppresses the reticular activating system and monoaminergic neuronal activity. This network causes a functional disconnection of sensory input to the cortex and decreases the metabolic rate of most of the cortex. During stage N3, cortical neuronal synchrony is promoted, and this may be related to synaptic pruning. REM sleep, however, is an activation of cholinergic neurons in the pontine dorsal tegmentum that subsequently excite neurons responsible for REM-associated atonia, REMs, increase in cortical metabolic rate, loss of thermoregulation, and other features. REM sleep is inhibited by activation of the dorsal raphe and locus ceruleus. A network of neurons in the hypothalamus midbrain and thalamus seems to regulate REM sleep cycling.
Hypocretin—named so because it structurally resembles secretin in the gut—appears to stabilize the ability to remain awake. It is also referred to as orexin codiscovered by another group—named so because of its ability to stimulate food intake (from the Greek orexis meaning appetite).
Throughout the 24-hour day, the human body has a symphony of endocrinologic and metabolic variations that are timed to maximize performance during wakefulness and promote quality rejuvenation during sleep. Because we evolved on a planet that rotates every 24 hours, we developed a delicate neurochemistry anticipatory cycle that prepares the body for the upcoming sleepwake state. This circadian cycle is approximately 1 day as captured in the Greek meaning of circadian. Many body functions, including body temperature, plasma and urine hormones, renal functions, psychological performance measures, and internal sleep-stage organization, participate in this circadian rhythm. Humans have a circadian rhythm that is approximately 24.3 hours and is driven by the suprachiasmatic nucleus. This nucleus is influenced by external time clues to synchronize the body clock with the outside world, including bright light, activity, meals, and social interactions. Evidence for the importance of circadian rhythms comes from studies of acute phase shifts, such as those that occur after jet lag or shift work. Because our internal clock is longer than 24 hours, adaptation is slower after an eastward flight (phase advance) than after a westward flight (phase delay).
FIGURE 114.1 Stages of sleep. Each 30-second recording represents a different stage of sleep. Wake (W), NREM is divided into three stages (N1, N2, N3) and REM (R). For each recording, the top two channels are electro-oculogram (LOCA2 and ROC-A1); the following six are EEG, followed by chin EMG and leg EMG (LAT1-LAT2), airflow, chest and abdominal movements, ECG, and oxygen saturation.
FIGURE 114.2 Hypnogram. Graphical representation of sleep stages as a function of time. This hypnogram shows normal sleep architecture with the majority of slow-wave sleep in the first third of the night, REM sleep majority in the last third of the night, and progressive longer durations of REM.
SPECIFIC DISORDERS OF SLEEP
Diagnostic procedures are discussed in Chapter 29.
Nearly all patients with disorders of the central nervous system (CNS) are at high risk for sleep dysfunction, which may be a direct result or a secondary effect of the neurologic condition. Sleep disorders may exacerbate the symptoms of the underlying neurologic disorder and impair quality of life. In this chapter, we describe selected disorders. Fatal familial insomnia, a prion disease, is discussed in Chapter 68. Sleep-associated headache disorders and epilepsy syndromes are also discussed in their respective chapters.
INSOMNIA
Insomnia can consist of difficulty falling asleep (sleep-onset insomnia), difficulty staying asleep (sleep maintenance insomnia), both, or sleep that is nonrefreshing or nonrestorative. The daytime symptoms include excessive fatigue, impaired performance, or emotional change. Most people have an occasional night fraught with difficulty falling asleep or trouble maintaining sleep, usually caused by an alerting response to short-term stress; this is a normal property of the brain and is not considered insomnia if it resolves quickly. In the past, insomnia has been categorized into primary or secondary types but these were difficult to reliably ascertain. Insomnia is now considered as short-term, chronic, or other [Level 1].1
Short-term insomnia lasting less than 3 months duration might be closely linked to the surrounding events, psychological disturbances, or sudden changes in a medical condition. Typically, there is an identifiable precipitant that an individual is able to recall. Individuals may complain of disturbances fewer than three times per week but this results in a general dissatisfaction in their quality of sleep. It may also result in the individual catastrophizing that they may never sleep again. The 1-year prevalence of short-term insomnia is around 20% in the general adult population. Circadian rhythm disorders should be considered as mimickers of insomnia. In delayed sleep phase syndrome, individuals typically complain that they cannot fall asleep until later in the night and due to morning commitments have to curtail their sleep, and this results in sleep deprivation. Early morning arousal raises the possibility of advanced sleep phase if the patient falls asleep early in the evening.
Chronic insomnia, lasting greater than 3 months on 3 or more days per week, is usually attributed to multiple factors. The factors may be divided into predisposing, precipitating, and perpetuating, which outline the formation of insomnia as an ongoing process. Characteristics that predispose an individual for insomnia are female gender, older age, psychiatric or chronic medical illness, lower socioeconomic status, poor education, obsessive-compulsive nature, poor coping strategies, and hyperalertness (Table 114.1).
Insomnia may be precipitated by sudden changes in environment or challenges to the body or mind. These challenges may come in the form of acute medical illness, psychological or psychiatric events, shift in schedule, or changes in medications or supplements. After the start of the insomnia, patients adopt behaviors or rituals that perpetuate the insomnia. Patients may use maladaptive habits that occur during the day or night and include heavy caffeine or alcohol use; watching television, working, or playing video games while in bed; or even eating or exercising during the usual sleep period. They may become dependent on certain somnogenic substances. Some patients develop associations of not sleeping with the bedroom and may fear going to bed. These poor associations and expectations of poor sleep promote the apprehension toward sleep. The insomnia symptom complex may indicate an underlying disorder related to primary failure of the sleep mechanism or one in which sleep disruption is a result of another disorder. Patients with obstructive sleep apnea, restless legs syndrome, and even narcolepsy may complain of insomnia. Sleep diaries, accounting bedtime and wake time, can be useful in determining potential links to schedule or circadian rhythm issues. Perception of good sleep is an important factor in evaluating the complaint of insomnia.
TABLE 114.1 Principles of Good Sleep Hygiene Are the Basis for a Sound Night of Sleep
Principles of Sleep Hygiene
Establish regular bedtimes.
Wake regularly at a fixed time.
Regulate the amount of sleep obtained each night.
Exercise daily and regularly (particularly aerobic) but not in the late evening.
Sleep in a quiet, cool, comfortable environment.
Avoid caffeinated beverages and other stimulants (including tobacco) especially close to bedtime.
Avoid alcohol within 3 h of bedtime.
Avoid hypnotic drugs.
Do something relaxing before bedtime.
Some patients exaggerate their symptoms, whereas other patients may not perceive they are asleep. These individuals display the normal physiologic parameters of sleep but do not recognize that they have slept. This is referred to as sleep-state misperception or paradoxical insomnia.
Insomnia may also be produced by medical or neurologic disorders. Derangement of almost any system in the body can disrupt sleep. Patients with diseases affecting the nervous system, heart, liver, kidneys, gastrointestinal tract, or lungs commonly complain of insomnia. Musculoskeletal discomfort such as in arthritis or other rheumatologic disorders may become worse with periods of rest. Pain from entrapment neuropathies such as carpal tunnel are typically worse at night, and headaches such as cluster headache or pain related to increased intracranial pressure or brain mass lesions can become more intense during sleep. Nearly all of the psychiatric illnesses have some link to poor sleep. Patients with depression or anxiety disorders may have insomnia years prior to the presentation of the affective component. Although a causal relationship is still in debate, the association is clear. Insomnia may also herald the onset of psychosis or mania.
Treatment of insomnia should be directed toward symptom improvement and avoidance of maladaptive behaviors. Therapy for neurologic and psychiatric disorders should be optimized, and a multipronged approach addressing the patient’s behaviors, psychological attitudes, and the potential underlying neurochemistry should be constructed. Cognitive behavioral therapy for insomnia (CBT-i) consisting of sleep restriction therapy, relaxation therapy, stimulus control, and sleep hygiene (see Table 114.1) provides a solid therapeutic foundation. CBT-i is the most effective longterm therapy for insomnia. The use of acupuncture for insomnia remains equivocal due to the lack of methodologic consistency in the trials [Level 1].2
There are also a number of safe, effective hypnotic substances that may be used particularly in short-term insomnia to help restore normal sleep patterns and reverse negative associations with sleep time and the bedroom environment. These differ mainly in half-life, with zaleplon (5 to 20 mg) very short acting, zolpidem (5 to 10 mg) short, and eszopiclone (1 to 3 mg) the longest (therefore most useful in sleep maintenance insomnias). Ramelteon (8 mg) is a melatonin agonist that is also a mild hypnotic. Suvorexant (5 to 20 mg), a nonselective orexin antagonist was approved in 2014 for insomnia. When these agents fail, benzodiazepines and sedating antidepressant drugs are alternatives. Short-acting benzodiazepines are usually preferable to avoid daytime sedation, although if anxiety is also present, longer acting compounds can be useful. Many medications are used offlabel for insomnia particularly if there are concomitant symptoms that could be effectively treated at the same time, such as headaches or depression. Many medications typically used for insomnia have not received formal approval by the U.S. Food and Drug Administration (FDA) because they have not applied for insomnia as a specific indication. Substances that promote alertness should be minimized when possible, and additional medicinal therapy should be directed toward a specific disease process. The goal of treatment with any hypnotic should be to help restore normal sleeping patterns, followed by slow elimination of the drug (Table 114.2).
TABLE 114.2 A List of Current Medications Approved by the U.S. Food and Drug Administration for Insomnia
Available as oral, oral spray, and sublingual forms
Zolpidem ER
6.25-12.5
1.4-3.6
Women metabolize zolpidem at a lower rate than men.
Eszopiclone
1-3
5-7
—
Orexin antagonist
Suvorexant
5-20
8-14
—
Benzodiazepines
Estazolam
0.5-2
10-24
—
Flurazepam
15-30
47-100
—
Quazepam
7.5-15
47-100
—
Temazepam
7.5-30
8-20
—
Triazolam
0.0625-0.125
1.5-5.5
—
Tricyclic antidepressants
Doxepin
3-6
8-24
Approved in low-dose 3- and 6-mg formulations only
Selective melatonin receptor agonist
Ramelteon
8
8
—
Many others are used off-label.
FDA, U.S. Food and Drug Administration.
When an individual has less sleep than what is generally considered normal, concern may arise from those around them. Some individuals are short sleepers requiring less than 6 hours of sleep but do not complain of sleep/wake disturbances and therefore are not insomniacs per se. Others may spend excessive amounts of time in bed. This pattern may occur, for example, from parents allocating too much time for their children to sleep, but the child functions normally. Some adult individuals are long sleepers, requiring 10 or more hours of sleep to function without signs of sleep deprivation. Although frustrating to patients, this condition is best treated with longer sleep times so long as no other source of ineffective sleep is found.
THE HYPERSOMNIAS
Sleepiness is defined as the propensity to enter sleep. This is a normal feeling as one approaches a typical sleep period, but excessive sleepiness occurs when one enters sleep at an inappropriate time or setting. Excessive sleepiness can occur in degrees. In mild sleepiness, one might have only limited impairment, such as falling asleep while reading a book. Greater degrees of sleepiness, however, may be associated with bouts of irresistible sleep or sleep attacks that intrude on such activities as driving, having a conversation, or eating meals. This degree of sleepiness places the patient at significant risk for accidents and has a major impact on the person’s well-being. It must occur for at least 3 months prior to diagnosis.
Clinicians should always question their hypersomnic patients for clues of potential sleep debt, sleep disorders, or other medical or psychiatric causes. Sleep deprivation is the most common cause of sleepiness. Information regarding sleep habits, schedule during the week and weekends, and environment often discloses other important contributing factors. Excessive sleepiness may result from a wide range of medical disorders and medications. Patients with heart, kidney, or liver failure or rheumatologic or endocrinologic disorders such as hypothyroidism and diabetes may note sleepiness and fatigue. Neurologic disorders such as strokes, tumors, demyelinating diseases, epilepsy, and head trauma can evoke excessive sleepiness. Sleepiness is frequently the cardinal symptom of many sleep disorders (Table 114.3). Patients with sleep apnea, narcolepsy, restless legs syndrome-periodic limb movements, or even parasomnias may note excessive daytime sleepiness as their main complaint. Thus, the clinician should question the patient further to elucidate potential etiologies.
About 2% of men and 1.5% of women report sleeping at least 10 hours per night and are regarded as long sleepers (in children, it is 2 hours more than the age-specific normative data). The additional sleep time is spent in REM and N2 compared to other individuals. Providing that these individuals obtain sufficient sleep prior to testing, the multiple sleep latency test (MSLT) is normal.
Narcolepsy
Narcolepsy is an incurable lifelong neurologic disorder characterized by the tetrad of (1) excessive daytime sleepiness, (2) cataplexy, (3) sleep paralysis, and (4) hypnagogic hallucinations. Patients with narcolepsy also typically have fragmentation of nocturnal sleep. Estimates of prevalence range between 2 and 10 per 10,000 individuals in North America and Europe. It is about five times more prevalent in Japan, and the incidence is only 1 per 500,000 in Israel. The symptoms of narcolepsy typically present between ages 10 and 30 years, although cases have been reported with onset as early as age 2 years and as late as 76 years. Men and women are equally affected. There appears to be a bimodal distribution occurring in teenage years and later around age 35 years. Symptoms gradually develop over several years but once it has fully developed, there is usually only a minor fluctuation in the severity. Sleepiness is often minimized or thought to be related to other causes, and diagnosis can be delayed for years or even decades. As weight gain and depression are common other causes for excessive daytime sleepiness in a previously well-rested individual should be considered.
TABLE 114.3 Differential Diagnosis of Excessive Daytime Sleepiness