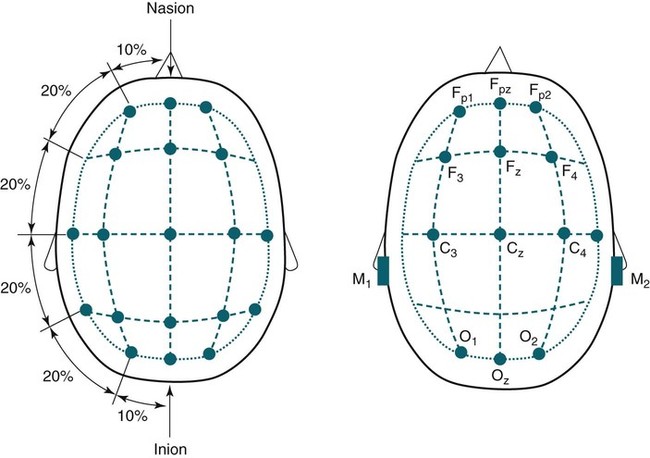
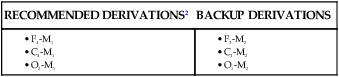
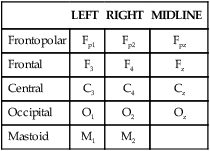
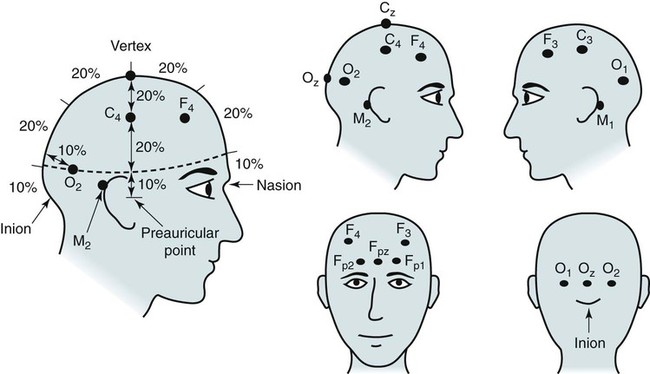
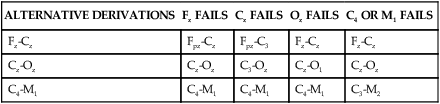
• In the EEG or EOG derivation G1-G2, an upward deflection in the tracing is noted if input G1 becomes negative with respect to input G2 (negative upward polarity). • To differentiate whether alpha waves or sleep spindles are present, change to a 10-second window and count the individual deflections in one second (see Fig. 1–3). • K complexes and slow waves have the greatest amplitude in frontal derivations. Sleep spindles and saw-tooth waves have the greatest amplitude in central derivations. • Alpha activity is any wave form with a frequency of 8 to 13 Hz. Alpha rhythm has a frequency of 8 to 13 Hz, is most prominent in the occipital derivations, and is enhanced by eye closure and attenuated by eye opening. • The recommended EEG derivations are F4-M1, C4-M1, and O2-M1. • The recommended EOG derivations are E1-M2 and E2-M2. Both eye electrodes are referred to a common mastoid electrode M2. • The front of the eye (cornea) is positive with respect to the back of the eye (retina). If the eyes move toward E1-M2 and away from E2-M2, this causes a downward deflection in E1-M2 and an upward deflection in E2-M2. • In the recommended EOG derivations, eye movements result in out-of-phase deflections. K complexes result in in-phase deflections. • In stage R, the chin EMG amplitude is equal to or lower than the lowest level in NREM sleep. The chin EMG activity can reach the REM level during NREM sleep. Transitions from NREM to stage R are not always associated with a drop in chin activity. Chin EMG activity is useful in differentiating stage R from stage W with the eyes open (REMs present). Sleep is divided into non–rapid eye movement (NREM) and rapid eye movement (REM) sleep. Sleep staging is based on electroencephalographic (EEG), electro-oculographic (EOG), and submental (chin) electromyographic (EMG) criteria. EOG (eye movement recording) and chin EMG recordings are used to detect REM sleep, which is characterized by REMs and reduced muscle tone. Since 1968, sleep was usually staged according to A Manual of Standardized Terminology, Techniques and Scoring System for Sleep Stages of Human Subjects, edited by Rechtschaffen and Kales (R&K).1 In the R&K scoring manual,1 NREM sleep was divided into sleep stages 1, 2, 3, and 4. REM sleep was referred to as stage REM. Sleep stage nomenclature has changed following the publication of the American Academy of Sleep Medicine (AASM) Manual for the Scoring of Sleep and Associated Events (hereafter referred to as the AASM scoring manual).2 The new nomenclature was introduced to denote sleep stages defined by new criteria. The old and new nomenclatures are shown in Table 1–1. Stages 3 and 4 are combined into stage N3. TABLE 1–1 AASM = American Academy of Sleep Medicine2; NREM = non–rapid eye movement; R&K = Rechtschaffen and Kales A1; REM = rapid eye movement; stages 3 and 4 are combined into stage N3. Monitoring to detect the presence and stage of sleep requires only a portion of the electrodes used in standard clinical EEG recording (Table 1–2). The nomenclature for the EEG electrodes follows the International 10–20 system.3 The “10–20” refers to the fact that the electrodes are positioned at either 10% or 20% of the distance between landmarks. The major landmarks include the nasion (bridge of the nose), inion (prominence at base of the occiput), and preauricular points (Figs. 1–1 and 1–2). In the 10–20 system, even-numbered subscripts refer to the right side of the head and odd-numbered subscripts to the left. Electrodes are named for the part of the brain they are over. For example, Fp1 and Fp2 are the left and right frontal pole electrodes, F3 and F4 are the left and right frontal electrodes, C3 and C4 are the left and right central electrodes, and O1 and O2 are the left and right occipital electrodes. Electrodes in the midline in the frontopolar, frontal, central, and occipital regions are named Fpz, Fz, Cz, and Oz, respectively. The position of the electrode Cz is at the top of the head and is called the vertex. The left and right mastoid electrodes in the new AASM scoring manual nomenclature are named M1 and M2, respectively. They were previously named A1 and A2. The nomenclature of EEG electrodes used for sleep monitoring is listed in Table 1–2. TABLE 1–2 Electroencephalographic Electrode Nomenclature EEG signals are displayed as voltage differences between two electrodes. The term derivation refers to a set of two electrodes (and the voltage difference between the electrodes). The term montage refers to a particular set of derivations. In sleep monitoring, electrodes in the frontal, central, and occipital electrodes are referenced against the opposite mastoid electrode. The AASM scoring manual recommends that all of the following electrodes be placed (F3, F4, C3, C4, O1, O2, M1, and M2). The recommended derivations and the alternative derivations are listed in Table 1–3. The backup derivations are displayed if one of the electrodes in the recommended derivation fails. For example, if electrode F4 fails, the derivation F3–M2 is used. In digital recording, one can easily display all six derivations if desired at the same time. In the original R&K scoring manual, only central derivations were utilized. However, additional derivations allow better visualization of the EEG patterns used to stage sleep. Although the derivations cited previously are the most widely used, the AASM scoring manual lists alternative acceptable derivations (Table 1–4). The alternative derivations use the electrodes Fz, Cz, Oz, C4, and M1 with the backup electrodes Fpz (to replace Fz), C3 (to replace Cz or C4), O1 (to replace Oz), and M2 (to replace M1). TABLE 1–4 Alternative Electroencephalographic Derivations with Backup Derivations It is common to place additional electrodes beyond those discussed in the AASM scoring manual to serve as a ground electrode and common reference. In sleep monitoring, a ground electrode is usually placed at or near Fpz and connected to the ground (or iso-ground) input on the electrode box. As discussed in Chapter 2, the ground is used to balance the individual AC differential amplifiers. One electrode (or two linked electrodes) is also placed to serve as a reference for referential recording (see Chapter 2). The reference electrode is commonly placed at or near Cz depending on which EEG electrodes are to be recorded for sleep monitoring. Recognition of certain characteristic EEG patterns is essential for sleep staging.1–6 EEG activity is recorded using a differential AC amplifier such that the signal recorded is the difference in voltage between two inputs (G1 and G2). By EEG convention, if input G1 is negative with respect to G2, this results in an upward deflection. As noted previously, the term derivation is used to describe the differential signal between two inputs. For example, in the derivation C4-M1, a change in the voltage between these electrodes results in an upward deflection if C4 is negative with respect to M1. EEG activity is described by frequency in cycles per second (hertz = Hz), amplitude (microvolts [µV]), and shape. The classically described EEG frequency ranges are delta (<4 Hz), theta (4–7 Hz), alpha (8–13 Hz), and beta (>13 Hz). Activity that is faster results in narrower deflections and slower frequency results in wider deflections. Sharp waves are narrow waves of 70 to 200 msec duration and spikes have a shorter duration of 20 to 70 msec. Some of the characteristics of EEG patterns important for sleep staging are listed in Tables 1–5 through 1–9. In addition to frequency, the region of highest activity (amplitude) and the effects of maneuvers on the EEG activity are also important. For example, one could use the term “alpha activity” to describe any EEG activity with a frequency in the alpha range (8–13 Hz). However, alpha rhythm consists of activity most prominent in occipital derivations that is attenuated by eye opening and increased by eye closure (Fig. 1–3). An important part of biocalibrations (see Chapter 4) at the start of sleep recording is to ask patients to close and then open their eyes to document that they produce alpha rhythm. Bursts of alpha waves can also occur during stage R typically at a frequency 1 to 2 Hz slower than during wakefulness. TABLE 1–5 Characteristics of Alpha Rhythm and Sleep Spindles
Sleep Stages and Basic Sleep Monitoring
R&K
AASM
Wake
Stage W
Stage W
NREM
Stage 1
Stage 2
Stage 3
Stage 4
Stage N1
Stage N2
Stage N3
REM
Stage REM
Stage R
Eeg Electrode Placement
LEFT
RIGHT
MIDLINE
Frontopolar
Fp1
Fp2
Fpz
Frontal
F3
F4
Fz
Central
C3
C4
Cz
Occipital
O1
O2
Oz
Mastoid
M1
M2
EEG Derivations
ALTERNATIVE DERIVATIONS
Fz FAILS
Cz FAILS
Oz FAILS
C4 OR M1 FAILS
Fz-Cz
Fpz-Cz
Fpz-C3
Fz-Cz
Fz-Cz
Cz-Oz
Cz-Oz
C3-Oz
Cz-O1
Cz-Oz
C4-M1
C4-M1
C4-M1
C4-M1
C3-M2
EEG Patterns