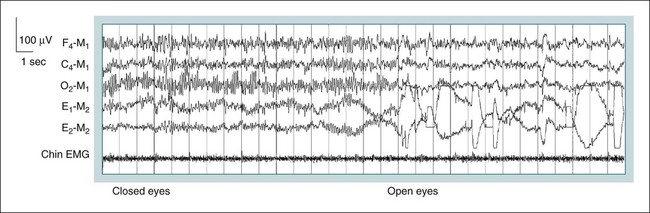
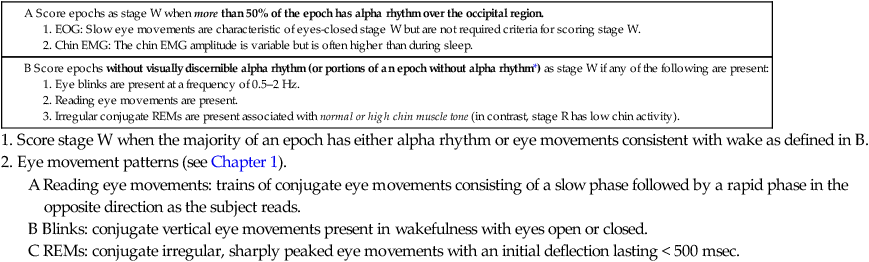
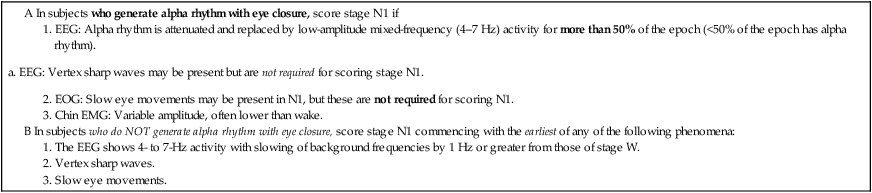
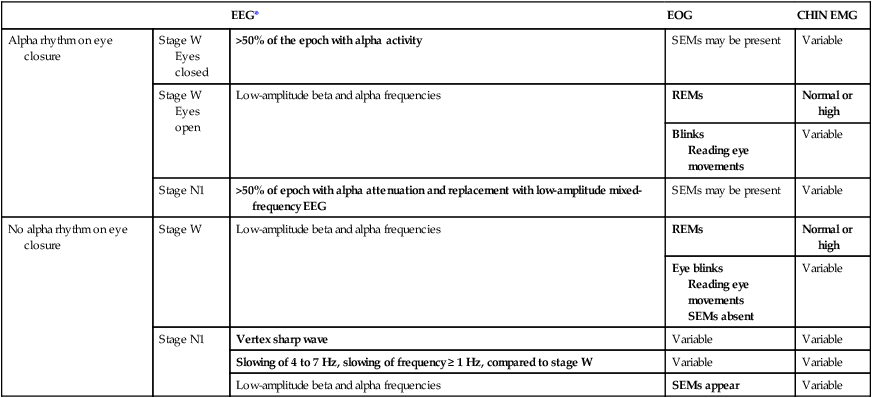
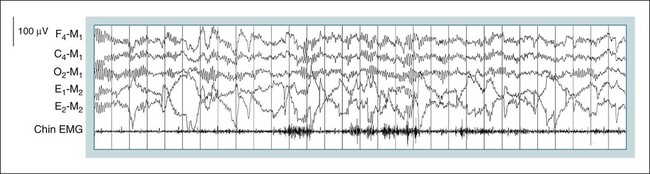
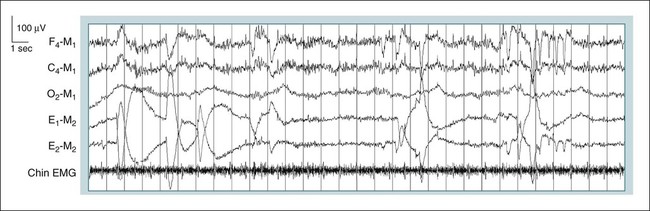
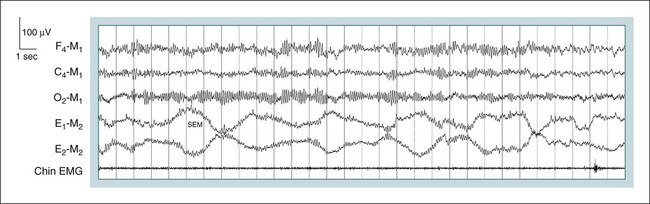
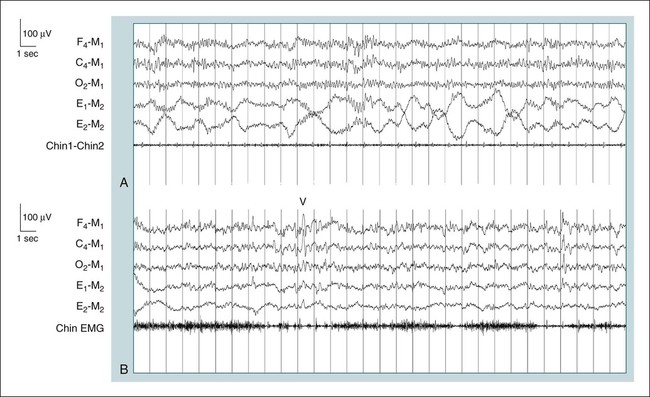
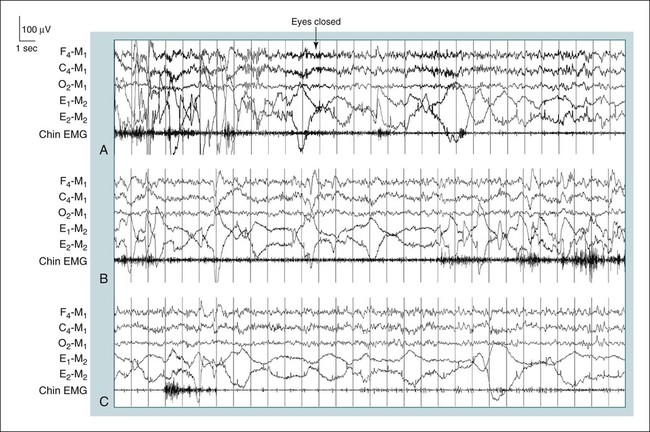
• The AASM scoring manual uses new nomenclature for wake and sleep (stages W, N1, N2, N3, and R). Stage N3 replaces stages 3 and 4 and stage R replaces stage REM. • Sleep is scored in sequential 30-second epochs. If more than one sleep stage occurs in an epoch, the epoch is scored based on the sleep stage occupying the majority of the epoch. • The 3-minute rule for stage N2 is no longer used. • The scoring of stage N3 is based on slow wave activity in the frontal derivation. • If subjects do not generate alpha rhythm on eye closure, the onset of stage N1 is based on the earliest occurrence of slow eye movements, EEG activity in the 4 to 7 Hz range with slowing of the background frequency by ≥ 1 Hz compared to wake, or vertex sharp waves. • The AASM scoring manual provides specific rules for scoring intervening epochs between epochs of definite stage N2 and definite stage R. The scoring manual does not provide rules for transitions between stage W and stage R or between stage N1 and stage R. Based on FAQ V7, begin scoring stage R when an epoch of definite stage R is present (contains both low EMG tone and REMs). From 1968 to 2007, sleep was staged according to the manual by Rechtschaffen and Kales (R&K).1,2 In the R&K manual, only central derivations were used to stage sleep, the term “movement time” was utilized to characterize epochs in which the electroencephalographic (EEG) and eye movement tracings are obscured by patient movement, and there was a 3-minute rule for the continuation of stage 2 (now known as stage N2). The AASM Manual for the Scoring of Sleep and Associated Events3,4 was published in 2007 (subsequently referred to as the “AASM scoring manual”). This manual changed the rules of staging sleep and made recommendations about the methods used to monitor sleep. The AASM scoring manual uses new nomenclature (Table 3–1) for the sleep stages, uses frontal and occipital as well as central EEG derivations, does not use the term “movement time,” and has no 3-minute rule for stage N2 sleep. In addition, stages 3 and 4 are combined into stage N3. The succeeding discussion follows the new rules with some minor adaptations for brevity and clarity. Answers to questions posed to the AASM Scoring Manual Steering Committee and clarifications of the staging rules are posted in a frequently asked questions (FAQs) document on the internet (http://www.aasmnet.org/Resources/PDF/FAQsScoringManual.pdf). The definitions of the EEG and eye movement patterns used for scoring are discussed in more detail in Chapter 1. TABLE 3–1 Comparison of R&K and the American Academy of Sleep Manual *Rechtschaffen A, Kales A (eds): A Manual of Standardized Terminology Techniques and Scoring System for Sleep Stages of Human Sleep. Los Angeles: Brain Information Service/Brain Research Institute, UCLA, 1968. †Iber C, Ancoli-Israel S, Chesson A, Quan SF for the American Academy of Sleep Medicine: The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications, 1st ed. Westchester, IL: American Academy of Sleep Medicine, 2007. During wakefulness, patients make the transition from full alertness to the early stages of drowsiness. During eyes open stage W (Fig. 3–1), the EEG consists of low-amplitude activity (chiefly beta and alpha frequencies) without the rhythmicity of alpha rhythm (8–13 Hz most prominent over occipital derivations). Often, muscle artifact (high-frequency activity) is also present in the EEG. Rapid eye movements (REMs) and eye blinks (vertical movements 0.5–2 Hz) may occur. The submental (chin) electromyogram (EMG) is usually relatively increased compared with that during sleep. The majority of individuals with eyes-closed stage W will demonstrate alpha rhythm most prominent in the occipital area. Slow eye movements (SEMs) may also be present and the chin EMG activity is relatively high. The rules for scoring stage W are listed in Table 3–2. In subjects who generate alpha rhythm, stage W is scored when more than 50% of the epoch contains alpha rhythm over the occipital region (see Table 3–2, rule A). SEMs may or may not be present during periods when alpha rhythm is present. Epochs without visually discernible alpha rhythm (see Table 3–2, rule B) are scored as stage W if any of the following are present: Eye blinks of a frequency of 0.5 to 2 Hz, reading eye movements, or irregular conjugate REMs with normal or high chin muscle tone. These eye movement patterns are characteristic of stage W. The requirement of normal or high chin EMG tone for REMs is because stage R (REM sleep) is characterized by REMs and low muscle tone. TABLE 3–2 B Score epochs without visually discernible alpha rhythm (or portions of an epoch without alpha rhythm*) as stage W if any of the following are present: 1. Score stage W when the majority of an epoch has either alpha rhythm or eye movements consistent with wake as defined in B. 2. Eye movement patterns (see Chapter 1). A Reading eye movements: trains of conjugate eye movements consisting of a slow phase followed by a rapid phase in the opposite direction as the subject reads. B Blinks: conjugate vertical eye movements present in wakefulness with eyes open or closed. C REMs: conjugate irregular, sharply peaked eye movements with an initial deflection lasting < 500 msec. EMG = electromyogram; EOG = electro-oculogram; REMs = rapid eye movements. *Adaptation of AASM scoring manual stage W, rule B. Adapted from Iber C, Ancoli-Israel S, Chesson A, Quan SF for the American Academy of Sleep Medicine: The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications, 1st ed. Westchester, IL: American Academy of Sleep Medicine, 2007. How should one score epochs that contain both portions with alpha rhythm (but < 50% of the epoch) AND portions with eye movements consistent with wake? The AASM scoring manual did not specifically address this situation. However, one can modify stage W rule B to apply to the portions of the epoch without alpha rhythm that contain eye movements consistent with wake (see Table 3–2, rule B). If the portions of the epoch containing alpha rhythm AND the portions of the epoch considered to be wake due to eye movements add up to more than 15 seconds (majority of the epoch), then the epoch is scored as stage W. Of note, approximately 10% of subjects do not generate alpha rhythm on eye closure and a further 10% may generate limited alpha rhythm. In these subjects, the occipital EEG activity is similar during eye opening and eye closure. When alpha rhythm is not generated with eye closure, the rules for scoring stage W and stage N1 are somewhat different and sleep onset is more difficult to define (Tables 3–3 and 3–4). In patients who do not generate alpha rhythm, epochs satisfying rule B in Table 3–2 are scored as stage W. Otherwise, epochs are scored as stage W if they do NOT meet criteria for stages N1, N2, N3, or R. In contrast to patients generating alpha rhythm, the presence of SEMs is a criterion for scoring stage N1 in subjects who do not generate alpha rhythm (see Table 3–4). TABLE 3–3 EEG = electroencephalogram; EMG = electromyogram; EOG = electro-oculogram. Adapted from Iber C, Ancoli-Israel S, Chesson A, Quan SF for the American Academy of Sleep Medicine: The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications, 1st ed. Westchester, IL: American Academy of Sleep Medicine, 2007. TABLE 3–4 Note: Bold text denotes essential features. *The EEG is assumed not to contain sleep spindles or K complexes not associated with arousal. In Figure 3–1, a 30-second tracing shows the transition from eyes-closed stage W to eyes-open stage W. Slightly more than 50% of the epoch contains alpha activity. Alpha activity is attenuated with eye opening and REMs are noted. In Figure 3–2, portions of the epoch contain alpha rhythm and other portions are considered stage W owing to the presence of eye movements consistent with wakefulness (see Table 3–2, stage W rule B). The majority of the epoch contains either alpha rhythm or eye movements consistent with wakefulness, and hence, the epoch is scored as stage W. In Figure 3–3, the chin EMG activity is relatively high, REMs and blinks are present, and there is no discernible alpha activity. The epoch is scored as stage W using stage W rule B (see Table 3–2). Figure 3–4 illustrates an example of eyes-closed stage W. Here, greater than 50% of the epoch has prominent alpha activity. SEMs are also present and the EMG activity is relatively decreased. It should be noted that SEMs can be seen during both eyes-closed stage W and stage N1. If patients produce alpha rhythm with eye closure, SEMs are not part of the criteria to score stage W (although they are characteristic during eyes-closed stage W). Low-amplitude mixed-frequency (LAMF) activity is defined as a low-amplitude EEG pattern with predominantly 4- to 7-Hz activity. Stage N1 is characterized by LAMF activity and the absence of sleep spindles (SSs) and K complexes (KCs) not associated with arousal. SEMs may occur (see Table 3–3). At the transition from stage N1 to stage N2, vertex sharp waves may appear. In patients who produce alpha activity with eye closure (stage N1 rule A, see Table 3–3), the onset of stage N1 occurs when more than 50% of the epoch is marked by alpha attenuation (alpha activity in < 50% of the epoch) and replacement with LAMF EEG (Fig. 3–5). In individuals who do not produce alpha activity with eye closure (Fig. 3–6), the start of stage N1 occurs at the earliest occurrence of SEMs, a slowing of the EEG by 1 Hz or more from that in stage W, or the presence of vertex sharp waves (stage N1 rule B, see Table 3–3). Table 3–4 displays the characteristics of stage W and stage N1 for patients who do and do not produce alpha with eye closure. As noted in the AASM scoring manual, because SEMs may occur before alpha attenuation in subjects who have alpha activity with eye closure, the sleep onset may be scored somewhat earlier in patients who do not produce alpha activity with eye closure. Stage N2 is characterized by the presence of one or more nonarousal KCs (i.e., KCs NOT associated with an arousal) or one or more trains of SSs (Fig. 3–7). Arousal rules are discussed later in this chapter. During epochs of stage N2, eye movements have usually ceased and the chin EMG is variable but usually at a level lower than that during wakefulness. Recall that a KC is said to be associated with an arousal (KC+Ar) if the arousal commences no more than 1 second after the termination of the KC. Also note that the KC activity is seen in the recommended electro-oculographic (EOG) derivations (E1-M2 and E2-M2) as in-phase deflections in contrast to REMs (out-of-phase deflections). The rules for scoring stage N2 are listed in Table 3–5 and summarized in Table 3–6. TABLE 3–5
Sleep Staging in Adults
R&K*
AASM SCORING MANUAL†
Stage W
Stage W
Stages 1, 2, REM
Stages N1, N2, R
Stages 3, 4
Stage N3
Central EEG derivations
Frontal, central, and occipital derivations
3-minute rule for continuation of stage 2 after an epoch with K complexes or sleep spindles
No time limit on stage N2 continuation
Movement arousal based on EMG—an increase in the EMG of any channel accompanied by a change in pattern of any additional channel
Arousal based on EEG (and chin EMG for stage R)
Movement time when EEG and EOG obscured for more than half the epoch
No movement timeMajor body movement rules
Scoring by Epochs
Stage W (Wake)
EEG*
EOG
CHIN EMG
Alpha rhythm on eye closure
Stage W
Eyes closed
>50% of the epoch with alpha activity
SEMs may be present
Variable
Stage W
Eyes open
Low-amplitude beta and alpha frequencies
REMs
Normal or high
Blinks
Reading eye movements
Variable
Stage N1
>50% of epoch with alpha attenuation and replacement with low-amplitude mixed-frequency EEG
SEMs may be present
Variable
No alpha rhythm on eye closure
Stage W
Low-amplitude beta and alpha frequencies
REMs
Normal or high
Eye blinks
Reading eye movements
SEMs absent
Variable
Stage N1
Vertex sharp wave
Variable
Variable
Slowing of 4 to 7 Hz, slowing of frequency ≥ 1 Hz, compared to stage W
Variable
Variable
Low-amplitude beta and alpha frequencies
SEMs appear
Variable
Stage N1
Stage N2
Related posts:
 Obstructive Sleep Apnea Treatment Overview and Medical Treatments
Obstructive Sleep Apnea Treatment Overview and Medical Treatments
 The Restless Leg Syndrome, Periodic Limb Movements in Sleep, and the Periodic Limb Movement Disorder
The Restless Leg Syndrome, Periodic Limb Movements in Sleep, and the Periodic Limb Movement Disorder
 Biocalibration, Artifacts, and Common Variants of Sleep
Biocalibration, Artifacts, and Common Variants of Sleep
 Insomnia
Insomnia
 Central Sleep Apnea and Hypoventilation Syndromes
Central Sleep Apnea and Hypoventilation Syndromes
 Cardiac Monitoring during Polysomnography
Cardiac Monitoring during Polysomnography
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Sleep Staging in Adults
