Chapter 78 Spinal Cord Injury
Epidemiology
Acute spinal cord injury occurs worldwide, with an annual incidence of 5–40 cases per million. The greatest frequency of spinal cord injuries is between ages 15 and 25 years, with a male to female ratio of 4:1. Common causes are motor vehicle accidents (50 percent), falls and work-related injuries (30 percent), violent crime (11 percent), and sports-related injuries (9 percent) [Rihn et al., 2009; Rowland et al., 2008]. In the United States and Canada, the annual incidence of traumatic spinal cord injury is 30–46 cases per 1 million population [Decker and Hergenroeder, 2004]. In the United States, 8000–12,000 new spinal cord injuries occur annually. Fewer than 10 percent of these patients die from their acute injuries [Bramlett and Dietrich, 2007; Walker, 1991], with 200,000–250,000 persons now living in the United States with sequelae of spinal cord trauma [Bramlett and Dietrich, 2007; Green and Eismont, 1984; Meyer et al., 1991; Oliver, 1992; Walker, 1991]. Pediatric patients constitute 0.3–13 percent of that number [Apple et al., 1995; Dias, 2004; Hadley et al., 1988; Hill et al., 1984; Proctor, 2002], with 3–5 percent of the spinal cord injuries that occur each year in the United States being found in persons younger than 15 years of age, and 20 percent in persons younger than 20 years of age [Vogel and Anderson, 2003]. The risk of spinal cord injury is equal for males and females from birth to age 3 years; the male to female ratio is 6:4 from age 4–8 years, 7:3 from age 9–15 years, and 8.5:1.5 from age 16–20 years [Massagli, 2000].
Of all pediatric trauma admissions to hospital, 1.5 percent involve the cervical spine. Motor vehicle-related accidents account for 48–61 percent of all pediatric cervical spine injuries. Falls account for 18–30 percent of cervical spine injuries below 8 years of age, and 11 percent over age 8 years [Gore et al., 2009]. Each year, 11,000 neck injuries, sustained while playing American football, present to emergency departments in the United States [Rihn et al., 2009]. Review of the National Pediatric Trauma Registry from 1988 to 1998 identified 75,172 injured children, of which 1.5 percent had a cervical spine injury. Eighty-three percent of the children had an injury of the bony spine, involving the upper cervical spine in 52 percent, the lower cervical spine in 28 percent, and both in 7 percent (13 percent unspecified). In 35 percent of the children, there was a spinal cord injury, that was incomplete in 76 percent and complete in 24 percent [Patel et al., 2001]. The National Trauma Data Bank (NTBD) was reviewed from 2001 to 2005 for children less than 3 years of age with a blunt cervical spine injury. Of 95,664 children below 3 years of age, 1.6 percent had a cervical spinal injury (bony spine and/or spinal cord). Although the most commonly fractured spine was C2, as has been found by others [Ruge et al., 1988], nearly half of all cervical spine fractures (47 percent) and more than half of the cervical spinal cord injuries (53 percent) were in the lower cervical spine (C5–7) [Polk-Williams et al., 2008]. The frequency of high cervical spinal injuries in very young children has been explained by the higher fulcrum of motion in younger children, and by weakness of C2 as a result of incomplete ossification of its synchondrosis [Proctor, 2002].
Motor vehicle accidents, including lap belt injuries to the lumbar spine, are the principal cause of spinal cord injuries, followed in decreasing order of frequency by falls, recreational or sports activities (especially diving accidents and football injuries), and penetrating injuries of the spinal column (e.g., gunshot, knife) [Gibson, 1992; Maroon et al., 1980; Massagli, 2000; Meyer et al., 1991; Mueller and Blyth, 1987; Schneider, 1964; Vogel and Anderson, 2003]. Since the 1980s, violence as a cause of spinal cord injury has increased from 10 to 30 percent in patients aged 16–20 years [Vogel et al., 1997]. Traumatic birth injury accounts for only 10–15 percent of all cases [Hadley, 1992]. Determinants of the severity of injury occurring after spinal cord trauma include the following:
The mortality from spinal cord injury in children is more than twice that seen in adults [Hamilton and Myles, 1992].
Anatomy
Bony Spine and Ligaments
The structure of the bony spine provides protection for and prevents excessive movement of the underlying spinal cord. Major ligaments that functionally divide the spine into anterior and posterior compartments maintain stability of the bony spinal column during movement [Chilton and Dagi, 1985]. Anteriorly, these ligaments are the anterior and posterior longitudinal ligaments; posteriorly, the ligaments include the ligamentum flavum and the interspinous, intertransverse, supraspinous, and facet capsular ligaments. Additionally, the transverse or cruciate ligament provides important stability between the atlas and axis. Stability of the spine as a whole is ensured if all of the anterior ligaments or if all of the posterior ligaments plus one anterior ligament are intact [Chilton and Dagi, 1985].
The most mobile portion of the spinal column is the cervical region, making that area the most common site of spinal cord injury [Green and Eismont, 1984; Hill et al., 1984]. Younger children are particularly susceptible to injuries of the high cervical cord [Davis et al., 1993; Piper and Menezes, 1996; Vogel et al., 1997]. Factors predisposing the upper cervical spine to injury in the young child include a proportionally larger and heavier head, relative underdevelopment of the neck muscles and ligaments, incomplete ossification of the vertebral bodies with relative anterior wedging [Massagli, 2000], incomplete development of the uncinate processes, smaller vertebral bodies of C1–C2 compared with C3–C5, and the more horizontal orientation of the articular surfaces of the cervical facet joints [Glasser and Fessler, 1996; Hadley et al., 1988; White and Panjabi, 1990]. Approximately 55 percent of spinal cord injuries involve the cervical spine, 30 percent involve the thoracic spine, and 15 percent involve the lumbar spine [Marion, 1998]. With birth trauma, spinal cord injuries are most common in the high cervical region (usually during an instrumental cephalic delivery) and in the lower cervical and upper thoracic regions (usually during a breech delivery). With increased use of cesarean sections to avoid potentially problematic vaginal deliveries, the frequency of spinal cord injury incurred during delivery has lessened appreciably [Morgan and Newell, 2001]. Between infancy and 8 years of age, 75 percent of spinal injuries occur in the cervical spine, particularly in its upper portion. Between age 8 and 14 years, 60 percent of injuries occur in the cervical spine, and 20 percent occur in the thoracic region, with the remainder at lower spinal levels [Menezes et al., 1989]. Conditions predisposing to cervical spinal cord injury in children include Down syndrome (15 percent have atlantoaxial instability), Klippel–Feil syndrome, Morquio’s syndrome, Larsen’s syndrome, achondroplasia, and previous cervical spine surgery [Caviness, 2004; Massagli, 2000].
The most common causes of cervical spine trauma in persons 18 years old and younger are motor vehicle accidents (45 percent), diving (23 percent), falls (11 percent), gymnastics (7 percent), football (5 percent), and other miscellaneous causes (8 percent) [Hill et al., 1984]. The second most mobile portion of the spine is the thoracolumbar region. It also is the second most commonly injured area, with T10 the site most frequently fractured [Ruge et al., 1988]. Regardless of the mechanism of injury, the thoracic spine (T2–T10) is the most common site of fracture in pediatric trauma patients [Reddy et al., 2003]. The thoracic and lumbosacral regions are the portions of the cord least often injured after trauma [Green and Eismont, 1984].
Spinal Cord
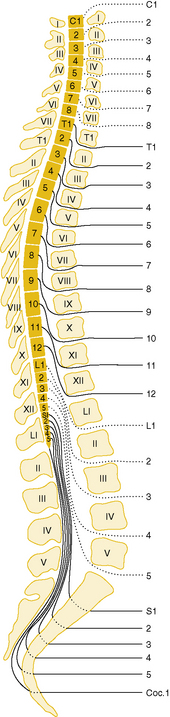
A disparity exists between vertebral and segmental cord levels, which changes with age. Early in fetal life, the spinal cord extends throughout the bony vertebral column, but during later development, the vertebral column becomes longer than the spinal cord. The caudal end of the cord comes to lie at successively higher vertebral levels; at birth, it is at the level of the second lumbar vertebra; in adulthood, it is at the first lumbar level. Disparity also exists between the levels of exit of nerve roots from the spinal canal and corresponding spinal segmental levels from which they originate, with the nerve roots emerging below their sites of origin (see Chapter 2). Below the first lumbar segment, there is no spinal cord, only the lumbosacral roots composing the cauda equina (Figure 78-1).
Blood Supply
The anterior spinal artery is an unpaired vessel formed by junction of a branch from the two vertebral arteries. It descends the entire length of the spinal cord ventrally in the anterior median sulcus. Between C3 and L3, the anterior spinal artery receives additional blood supply from anterior radicular arteries derived from lateral spinal arteries. Branches from the anterior spinal artery supply the entire anterior columns and most of the lateral columns of the spinal cord. The two posterior spinal arteries communicate with posterior radicular branches of the lateral spinal arteries to form a rich plexus of collaterals that supply the entire posterior columns and the remainder of the lateral columns of the spinal cord [Herren and Alexander, 1939; Suh and Alexander, 1939].
Pathogenesis: Mechanisms of Spinal Cord Injury
When the spinal cord sustains traumatic injury, the forces applied to the spine usually have been sufficient to cause displacement of vertebral ligaments and bones [Kakulas, 1984]. There are five major ways in which trauma to the spine can result in injury to the spinal cord: forward flexion, lateral flexion, rotation, axial compression, and hyperextension [Chilton and Dagi, 1985]. The forces generated by these movements can result in vertebral distraction, dislocation, fracture, and disc herniation. Often, as is the case in motor vehicle accidents and birth trauma, several forces act at the same time to injure the spine [Glasser and Fessler, 1996]. Osseous disruption (fracture or displacement) is the most common cause of spinal cord injury. Ligamentous injury, without osseous disruption, causing spinal cord injury is common in children, resulting in spinal cord injury without radiographic abnormality (SCIWORA). Disc herniation occurs in approximately 50 percent of spinal cord-injured patients [Flanders et al., 1990].
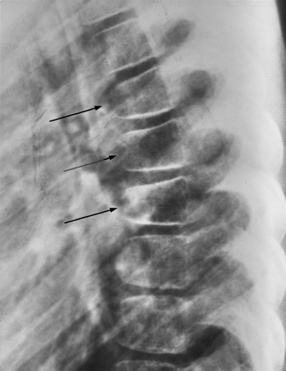
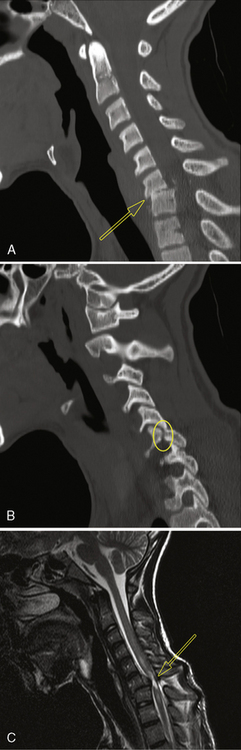
Forward flexion can lead to wedge or teardrop fractures, which usually begin at or near the intervertebral disc (Figure 78-2). These fractures are often encountered in motor vehicle accidents involving passengers not wearing seat belts, but also can be seen in children wearing ill-fitting adult types of lap-sash belts (cervical seat-belt syndrome) [Hoy and Cole, 1993]. Excessive lateral flexion of the cervical spine is always accompanied by rotation and can cause a unilateral locked facet (Figure 78-3). This locked facet occurs when the inferior facet contralateral to the side of flexion rotates too far anteriorly and locks into the superior facet of the vertebral body below [Panjabi and White, 1980]. Simple flexion alone usually causes little damage, but with the addition of rotation, ligaments can rupture, rendering the spine unstable and prone to distraction and dislocation. Rotation and flexion, accompanied by posterior ligamentous tear, also can cause vertebral body shear fractures.

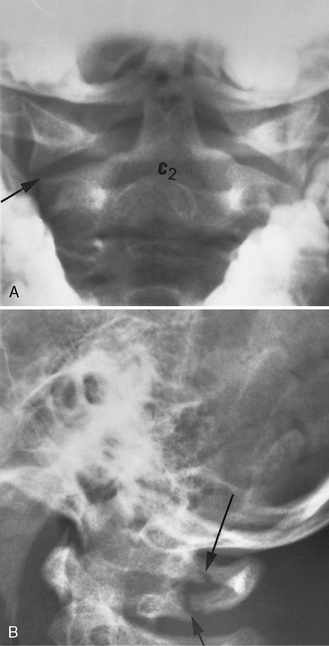
Axial compression typically occurs in diving accidents, falls, and sports injuries. Axial compression can result in a burst fracture in which the vertebral end plate is injured, allowing the intervertebral disc to rupture into the vertebral body, which then bursts. In the Jefferson fracture, a direct blow to the top of the head results in axial compression that is transmitted through the occipital condyles to the atlas, the arch of which bursts, allowing fragments to be displaced outward (Figure 78-4) [Shapiro et al., 1973]. Severe hyperextension is often encountered in rear-end motor vehicle accidents (whiplash injury) and in the head-shaking injury of child abuse. This hyperextension can result in transverse fractures of the neural arches of the cervical spine, usually accompanied by tearing of the anterior longitudinal ligament [Caffey, 1974; Janes and Hooshmand, 1965; Ommaya, 1969]. The so-called hangman’s fracture occurs from a hyperextension injury through the synchondrosis between the odontoid and the arch of C2 [Reynolds, 2000]. Because the vertebral arteries lie in the transverse processes of these vertebrae, they can be torn or thrombosed after such injuries, with resultant ischemia to the anterior two-thirds of the spinal cord. Such injuries have been reported after neck hyperextension in football games and in infants with C1–C2 instability [Gilles et al., 1979; Schneider et al., 1970]. Displacement of the vertebrae during spinal trauma can compress the arteries of the spinal cord, resulting in ischemic injury, often without radiographic abnormalities.
Neuropathology
The nature and severity of traumatic injury to the spinal cord are related to the type and location of vertebral damage, the presence of any pre-existing disorder affecting the size of the spinal canal or mobility of the spinal cord (e.g., spinal stenosis, spondylitis, prolapsed disc), and the occurrence of concomitant vascular injury [Braakman and Penning, 1976; Chilton and Dagi, 1985]. Pathologic examination after spinal cord trauma has disclosed injuries that are either intraspinal intramedullary (affecting the spinal cord primarily) or, less often, intraspinal extramedullary (affecting the spinal cord secondarily). Intraspinal intramedullary pathologies include concussion, ischemia, contusion, compression, laceration, and intramedullary hemorrhage [Jellinger, 1976]. Intraspinal extramedullary injuries include epidural, subdural, and subarachnoid hemorrhages; epidural abscess; arachnoid cyst; epidermoid tumor; herniation of the nucleus pulposus; and cauda equina injuries.
Intraspinal Intramedullary Lesions
Pathogenesis and Pathologies
In spinal concussion, there is a functional rather than pathologic disturbance, usually with return of function within hours [Tator, 1996]. Extravasation of potassium from neurons into the extracellular space, after direct injury of nerve cell membranes or secondary nerve cell damage from vascular disruption, is the most likely mechanism of spinal cord concussion. Ischemia of the spinal cord can occur from anterior spinal artery or other vascular compression during spinal cord trauma, but also can occur when the trauma does not involve the spinal cord directly. Hypotension, systemic shock, and vascular injury to the aorta or a vertebral artery are the most common causes of this type of injury. With compression of the anterior spinal artery, the anterior two-thirds of the spinal cord is affected, causing weakness and loss of pain and temperature perception, with preservation of proprioception and light touch. Contusion results from a blunt injury of the spinal cord without continued compression or disruption of nerve tissue, resulting in transient paresthesias and dysesthesias in the upper limbs, especially the hands (burning hands syndrome), accompanied by transient long tract signs. Recovery is incomplete, however, distinguishing contusion from concussion. Central cord necrosis (hemorrhagic or ischemic) is a common sequela that often can be seen on magnetic resonance imaging (MRI) [Bailes et al., 1991; Jellinger, 1976]. Compression of the spinal cord can be caused by vertebral dislocation or by pressure from bony fragments, a herniated disc, or extramedullary bleeding [Jellinger, 1976]. Laceration occurs when there is interruption of spinal cord tissue by bony fragments, knife or bullet wounds, fracture-dislocation, or severe stretching. In older children, the most frequent cause of laceration is a penetrating agent, whereas in newborns, hyperextension of the neck during breech delivery is the most likely cause [Allen et al., 1969; Bresnan and Abroms, 1974; Byers, 1975; Crothers, 1923]. Intramedullary hemorrhage, which can extend over several spinal cord segments (hematomyelia), is believed to result from direct injury to blood vessels or from altered vascular permeability, as from acidosis.
The pathology of intraspinal intramedullary injuries has been studied in detail in experimental animals and in human postmortem examination material [DeLaTorre, 1981; Dumont et al., 2001a; Jellinger, 1976; Kakulas, 1984; Norenberg et al., 2004; Park et al., 2004; Profyris et al., 2004]. To mimic most events that lead to various forms of human spinal cord injury, several experimental models have been developed, the most common being transection, compression, or contusion [Rosenzweig and McDonald, 2004]. Because there are striking pathophysiologic similarities between human spinal cord injury and experimental models of spinal cord injury, particularly in the rat, findings in experimental spinal cord injury are commonly extrapolated to human injury. Such extrapolation requires caution, however, because regulation of secondary events after spinal cord injury varies greatly among different animal species and strains [Profyris et al., 2004]. The pathologic changes observed in the spinal cord after trauma can be subdivided into early, late, and very late.
The pathophysiology of spinal cord injury is biphasic. First is the primary injury, which is mechanical (e.g., spinal fracture and/or dislocation), directly disrupting axons, blood vessels, and cell membranes. This is followed by the delayed onset of secondary injury, involving vascular dysfunction, edema, ischemia, excitotoxicity, electrolyte shifts, free radical production, inflammation, and delayed apoptotic cell death. While neurologic deficits are seen immediately following the initial injury, the secondary injury phase results in a protracted period of tissue destruction [Rowland et al., 2008].
Phases of secondary injury
Immediate Phase (0–2 Hours)
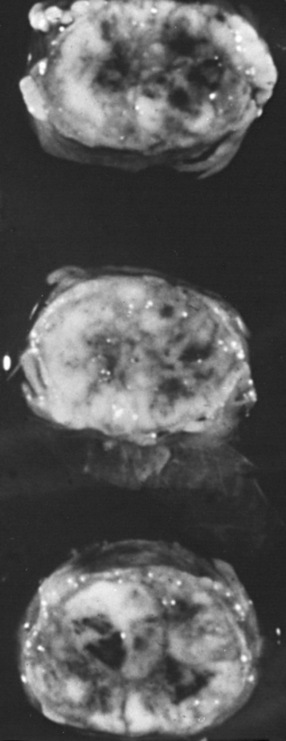
During the immediate phase of spinal cord injury, which can last for up to 2 hours, traumatic severing of axons, the immediate death of neurons and glia, and accompanying spinal shock result in immediate loss of function at and below the level of complete injury. Pathological changes consist of swelling of the spinal cord, often with hemorrhage in the central gray matter and surrounding white matter, and necrosis (Figure 78-5) and spinal cord ischemia extending for many segments rostral and caudal to the injury site. Activation of microglial cells begins almost immediately, with the upregulation of the proinflammatory cytokines tumor necrosis factor (TNF)α and interleukin (IL)-β, detectable within minutes of injury. Also within minutes, levels of extracellular glutamate can reach excitotoxic levels.
Acute Phase (2–48 Hours)
The acute phase of spinal cord injury lasts from 2 to 48 hours. It is characterized by continuing hemorrhage, increasing edema and inflammation, and the onset of additional secondary injury processes, including free radical production, ionic dysregulation, glutamate-mediated excitotoxicity, and immune-associated neurotoxicity, which cause vascular disruption, hemorrhage, and resulting ischemia, with further axonal injury and cell death. The ischemia results in cytotoxic cell swelling, affecting neurons and glia, and axonal swelling. Loss of ion homeostasis immediately following spinal cord injury and excitotoxicity both contribute significantly to the propagation of cell injury after spinal cord injury. Ion dysregulation is also a central feature of necrotic and apoptotic cell death. Excitotoxicity results from excessive activation of glutamate receptors and is believed to play a role in the death of neurons and glia. Production of free radicals gives rise to lipid peroxidation, contributing to axonal disruption and death of neurons and glia. The modest protective effect of methylprednisolone treatment following acute spinal cord injury is believed to be due, at least in part, to the inhibition of lipid peroxidation [Kwon et al., 2004]. An additional acute-phase change is a marked increase in permeability of the blood–brain barrier. Death of neurons at all stages of injury occurs mainly from necrosis; by contrast, oligodendroglia readily undergo apoptosis. Loss of oligodendroglia results in axonal demyelination; persistent demyelination and other forms of axonal injury can then cause death of associated cell bodies. Animal studies have provided strong evidence that spared demyelinated axons are present following contusive spinal cord injury, and represent an important therapeutic target for spinal cord injury treatments that either remyelinate (cell transplants) or improve axonal conduction in demyelinated fibers (4-aminopyridine) [Hayes et al., 2004; Nashmi and Fehlings, 2001]. On the other hand, postmortem human studies and a limited number of animal studies [Lasiene et al., 2008] have not convincingly shown significant numbers of spared demyelinated axons to be present after human spinal cord injury [Kakulas, 2004; Norenberg et al., 2004].
Chronic Phase (6 Months or More)
The chronic phase of spinal cord injury begins 6 months after injury and continues through the patients lifetime. Scar formation continues, and the central portion of the spinal cord is replaced by a cystic cavity extending for several segments above and below the point of impact, resulting in post-traumatic syringomyelia; this extension can continue over many years, significantly increasing the patient’s neurological deficit, including ascending paralysis, brainstem symptoms, and neuropathic pain [Barnett and Jousse, 1976; Profyris et al., 2004; Rowland et al., 2008; Tator, 1996]. Wallerian degeneration of ascending and descending tracts occurs within 6–12 months [Kakulas, 1999], and nerve roots at the level of the lesion become atrophic. The cord becomes thin in the area of injury, with fibrosis and thickening of the overlying meninges [Kakulas, 1984]. At this chronic phase, therapeutic strategies are directed to encouraging regeneration/sprouting of disrupted axons, promoting plasticity with rehabilitative strategies, and improving function of demyelinated axons. Despite much success with stem cell-based approaches when applied subacutely, use of stem cells during this chronic phase of injury has not been shown to be successful [Rowland et al., 2008].
Clinical Assessment
General Physical Examination
It is crucial to assess the entire child, even in the presence of an obvious spinal injury. Particular attention should be directed to the vital signs. Respiratory difficulty may be caused by a traumatic pneumothorax or by diaphragmatic paralysis consequent to injury of the midcervical spinal cord. Hypotension with tachycardia may result from intra-abdominal bleeding from a ruptured spleen. Temperature instability may accompany spinal shock. The entire spine, particularly the cervical portion, should be examined with great care. One should look for overlying bruising and any spinal deformity. While in-line immobilization of the spine, with particular attention to the neck, is maintained, the entire spine should be palpated for any point tenderness, deformities, crepitus, or muscle spasm [Kadish, 2001].
Neurologic Examination
The diagnosis of spinal cord injury is often overlooked in children with multiple injuries, unless constant vigilance to detect such injury is maintained. Spinal cord trauma should be suspected in cases of breech or otherwise difficult delivery; multiple trauma; child abuse; and certain sports injuries, such as football, gymnastics, and ice hockey [Braakman and Penning, 1976; Torg et al., 1979]. Patients with spinal cord injury can present with any combination of the following symptoms and signs: neck or back pain, weakness, sensory loss, decrease in deep tendon reflexes, loss of bladder or bowel control, autonomic dysfunction, and meningismus. Such symptoms may be classified further as acute, subacute, chronic, intermittent, delayed or late, or progressive. After the initial neurological deficit in acute spinal cord injury, secondary deterioration is sometimes seen. Such worsening can be:
Signs of spinal cord injury usually include impairment of motor and sensory function. The degree of motor involvement can vary from subtle weakness to complete paraplegia or quadriplegia. Loss of sensation is often ascertainable at an obvious dermatomal level. In 1992, the American Spinal Injury Association (ASIA) and the International Medical Society of Paraplegia (IMSOP) published a Standard Neurological Classification of Spinal Cord Injury (Figure 78-6). Such a classification offers a systematic documentation of motor, sensory, and sphincter function for the accurate classification and scoring of acute spinal cord injuries. Ten key muscle groups are tested for motor function, using the Medical Research Council 0–5 muscle grading system, and sensation is tested over 28 dermatomes on both sides of the body. The neurological levels and completeness or incompleteness (partial preservation) of spinal cord involvement are documented [American Spinal Injury Association, 1992].
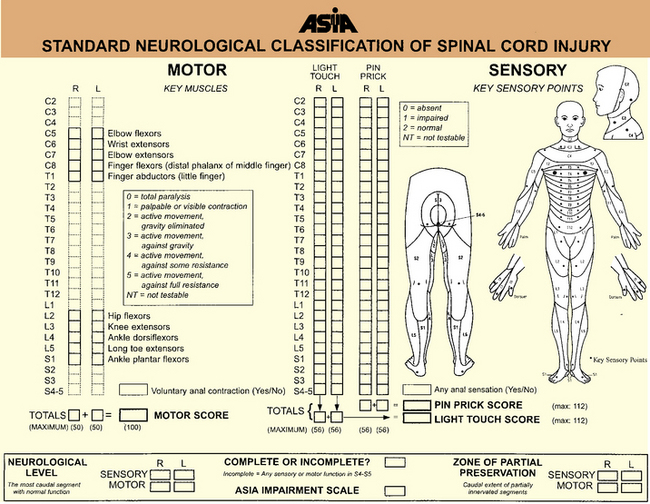
In 1992, the ASIA with the IMSOP developed the ASIA/IMSOP Spinal Cord Impairment Scale (Box 78-1) [Tator, 1996]. The ASIA/IMSOP scale incorporates the Medical Research Council muscle grading and pinprick/light touch sensory testing into a system differentiating complete and incomplete spinal cord deficit. Complete injury is defined as loss of all motor and sensory function in all segments below the neurological level, including the sacral dermatomes (S4–S5). To make this determination, peroneal and deep anal sensation and digital sphincter tone and contraction must be totally lacking. If there is preservation of any sensory or motor function below the neurological level, the injury is classified as incomplete (see Figure 78-6). Using this classification system, the examiner identifies the sensory and motor levels, defined as the most caudal spinal cord segment with normal sensory and motor function, on both sides. The zone of partial preservation is defined as the dermatomes caudal to the neurological level with partial preservation of function in an otherwise complete injury. A zone of partial preservation implies injury of multiple spinal cord segments, whereas its absence implies injury at only one level.
Box 78-1 American Spinal Injury Association/International Medical Society of Paraplegia Spinal Cord Impairment Scale*
Occasionally, brachial or lumbosacral plexus injuries causing weakness and sensory loss in a radicular distribution may coexist with a spinal injury, complicating the clinical picture. After injury to the spinal cord, the deep tendon reflexes are depressed or absent, with this lack of response persisting until the phase of spinal shock has resolved (1–12 weeks) [Green and Eismont, 1984; Guttmann, 1976; Meinecke, 1976]. Thereafter, hyperreflexia and extensor posturing are evident below the level of the lesion. Accompanying autonomic dysfunction can be manifested by Horner’s syndrome, hypertension, bowel and bladder atonia, and disturbances in temperature regulation.
Laboratory Studies
Radiographic Evaluation
Radiographic evaluation of the child suspected of having spinal cord injury should begin in the emergency department with plain films of the entire spine. The purpose of the evaluation is to look for evidence of unstable fractures or vertebral dislocations that may require emergency surgical intervention. Radiography of the entire spine is important because approximately 15 percent of patients have injury at multiple sites [Hadley, 1992; Hadley et al., 1988]. Radiological evaluation of the spine is often neither possible nor desirable in an emergency situation, however, and may need to be deferred until the spine is stabilized. In such circumstance, only the spinal area clinically involved needs immediate imaging. In cases in which the patient cannot be assessed adequately by plain radiography, MRI may be required early in the evaluation. Stringer and Andersen suggested a diagnostic algorithm for spinal injury combining the findings on neurological examination and results of radiographic studies [Andersen and Stringer, 1996; Stringer and Andersen, 1996].
Children with spinal cord injury routinely have sandbag and tape fixation of the head and neck, making optimal radiographic examination more difficult. Nonetheless, it is crucial to obtain anteroposterior, lateral, and oblique views of the spine. All seven cervical vertebrae and the C7–T1 interspace must be visualized. Swimmer’s views are often necessary to visualize all of the lower cervical vertebrae, and an open-mouth view may be needed to visualize the odontoid process [Goldberg et al., 1990], although the open-mouth view can be safely omitted if the other views are normal [Dias, 2004]. Flexion/extension cervical x-rays and fluoroscopy are sometimes indicated to exclude ligamentous instability when there is still suspicion of cervical spine instability after static x-rays have been obtained [Hadley, 2002b]. Care must be taken not to misinterpret normal variations in cervical spine films of a child. These variations include pseudosubluxation of C2 on C3 (seen in 20 percent of normal children age 1–7 years) and the cartilaginous plate at the base of the odontoid (normally seen in children <3 years old and often mistaken for a recent fracture) [Cattell and Filtzer, 1965].
Occipitoaxial dislocations can be identified on plain radiographs in some patients using the Powers ratio (distance of the basion [midpoint of the anterior border of the foramen magnum] to the posterior arch of C1, divided by the distance of the opisthion [midpoint of the lower border of the foramen magnum] to the anterior arch of C1). This ratio is usually 0.77. Ratios greater than 1 are abnormal. Most often, MRI is needed to identify occipitoaxial dislocations. Instability of the atlantoaxial region is suspected when the preodontoid space exceeds 5 mm in a child or 3 mm in an adult. Fractures of the atlas often can be stabilized by using a rigid (Philadelphia) collar [Alker et al., 1975]. Odontoid fractures and hangman’s fractures are rare in childhood and, if present, usually can be treated nonoperatively (halo brace) [Anderson and D’Alonzo, 1974].
Measurements made to assess alignment of the spinal column follow the “rule of 2”: that is, the allowable displacement between vertebrae in any direction should not exceed 2 mm in adults, with a greater allowance in children. The evaluation of bony integrity can be difficult at times, especially of the odontoid process and C1. If adequate quality cannot be obtained by plain radiographs, computed tomography (CT) is indicated [Andersen and Stringer, 1996; Stringer and Andersen, 1996].
Further limitations of plain radiographs of the spine include 40 percent false-positive and 20 percent false-negative interpretations. Also, significant spinal cord injury frequently occurs in children without radiographic abnormality (SCIWORA) (e.g., vertebral fracture or dislocation) [Burke, 1974; Pang and Wilberger, 1982], with this discrepancy observed in 15–70 percent of all pediatric spinal cord injuries [Hadley et al., 1988; Menezes et al., 1989; Pang and Wilberger, 1982]. Based on radiographic findings, spinal column injuries can be classified as follows:
SCIWORA, as first described, referred to cases of spinal cord injury with objective signs of myelopathy in the absence of abnormalities on static and dynamic flexion/extension films, CT imaging, and plain or CT myelography [Gore et al., 2009]. With modern MRI, many such cases show radiological evidence of injury to the spinal cord or spinal cord ligaments [Caviness, 2004; Davis et al., 1993; Matsumura et al., 1990; Proctor, 2002], with MRI abnormalities seen in about two-thirds of cases [Massagli, 2000]. Pang found MRI in 50 SCIWORA patients to have high prognostic value. The findings were complete transection or major hemorrhage (both with profoundly poor outcomes); minor hemorrhage (40 percent improved to mild disability); edema only (75 percent improved to mild disability); and normal (all recovered completely) [Pang, 2004].
Because the vertebral column in early life is quite elastic, allowing for significant flexion, hyperextension, and vertebral distraction without accompanying fracture or dislocations, SCIWORA is seen most often in infants and young children, in whom the frequency is three times greater than in children older than 10 years of age [Massagli, 2000]. Also predisposing to SCIWORA in young children is the greater elasticity of the spinal column than of the spinal cord; the bony spine can tolerate 5 cm of distraction, whereas the spinal cord can tolerate only 5 mm before disruption [Caviness, 2004]. Spinal cord ischemia from vertebral artery injury may also be contributory [Gore et al., 2009]. SCIWORA most often affects the cervical spine, typically producing signs of a central cord syndrome [Babcock, 1975]. In children less than 8 years, SCIWORA is more likely to be more rostral and more severe; from 8 to 16 years, it tends to be more caudal and less severe [Gore et al., 2009]. In some cases, transient neurologic symptoms may be the only indication that the cervical spinal cord has been injured; in other cases, permanent deficits may result, reflecting more severe spinal cord injuries that can be partial or complete [Caviness, 2004; Massagli, 2000]. In one study, 52 percent of children with SCIWORA had delayed onset of paralysis 4 days after their injury [Pang and Wilberger, 1982]. Children with spinal trauma must be examined frequently for signs of clinical deterioration in the days after their injury, even when plain radiographs of the spine are normal. Cervical immobilization of patients with SCIWORA is controversial. If dynamic films demonstrate stability of the cervical spine, the role of cervical immobilization is unclear. With only extraneural findings on MRI, neurological recovery, and no neck pain, 2 weeks of hard collar immobilization is recommended, followed by dynamic films; but with neural findings on MRI, the recommendation is for 12 weeks of hard collar immobilization before dynamic films are obtained [Gore et al., 2009]. Avoidance of high-risk activities for 6 months is recommended [Gunnarsson and Fehlings, 2003].
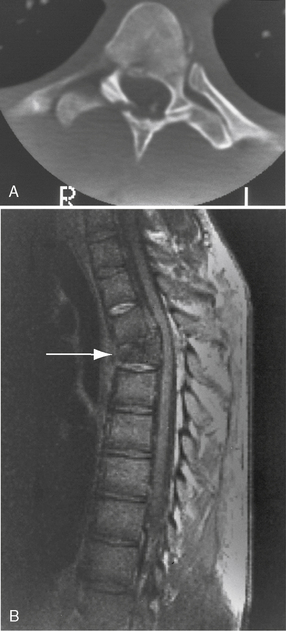
CT is the best means of detecting subtle spinal fractures and clarifying equivocal areas seen on plain films. CT also should be used when plain films are normal, but clinical suspicion of instability or fracture still exists [Andersen and Stringer, 1996; Stringer and Andersen, 1996], or when fracture/ displacement is seen on plain radiography [Caviness, 2004]. More recently, MRI of the spine has replaced CT and myelography as the preferred means of imaging the injured spinal cord (Figure 78-7) [Goldberg et al., 1988; Greenberg, 1991; Hyman and Gorey, 1988]. Many MRI sequences can be used, depending on the type of injury and the spinal cord area of concern, including spin-echo, fast-spin-echo, gradient-recall-echo, and inversion-recovery sequences. Excellent review articles on the use of these different sequences in specific situations are available [Andersen and Stringer, 1996; Stringer and Andersen, 1996]. MRI can distinguish intramedullary lesions from extramedullary ones, and early pathologic changes from later ones [Davis et al., 1993; Kalfas et al., 1988; Levitt and Flanders, 1991; Sett and Crockard, 1991]. In general, findings on MRI correlate well with the degree of deficit found on neurological examination [Bondurant et al., 1990; Davis et al., 1993; Flanders et al., 1990]. Additionally, the type and severity of spinal cord injury seen on MRI correlate well with the degree of recovery. In one study, MRI findings were classified into the following three categories:
 type I, inhomogeneous on T1-weighted image, large central hypointensity with thin hyperintense rim on T2-weighted image
type I, inhomogeneous on T1-weighted image, large central hypointensity with thin hyperintense rim on T2-weighted image

Neurological recovery was insignificant in patients with intraspinal hemorrhage, while patients with cord edema or contusion recovered significant neurological function [Kulkarni et al., 1987] (Figure 78-8).
In general, spinal cord injuries in which there is no identifiable MRI abnormality carry a better prognosis for recovery than injuries in which MRI abnormalities are found [Davis et al., 1993]. The usefulness of MRI in visualizing spinal cord injury in neonates, in whom neurologic abnormalities can be difficult to find and in whom significance can be difficult to interpret, has been documented [Lanska et al., 1990]. MRI also is useful in showing abnormalities that may not be seen with other imaging modalities, including ligamentous instability and disruptions, other soft-tissue injuries, disc herniations, intraspinal hemorrhage, and nerve root injuries [Kadish, 2001; Proctor, 2002]. In some cases, it may be necessary to use a combination of MRI and CT to identify coexisting injuries of the spinal cord and bony spine [Levitt and Flanders, 1991; Wittenberg et al., 1990]. MRI can be useful in predicting outcome in intramedullary lesions because it can differentiate hematoma (which often has a poor prognosis) from spinal cord edema, which usually has a better outcome [Schaefer et al., 1992]. In 49 patients who underwent MRI within 72 hours of sustaining a cervical spinal cord injury, the imaging features that correlated with a poor functional recovery included hemorrhage, long segments of edema, and high cervical lesions [Flanders et al., 1999].
Functional MRI has been used to assess the degree of spinal cord damage in 27 patients with complete and incomplete cervical and thoracic spinal cord injuries. With thermal stimuli applied to the inner calf (L4 sensory dermatome), activity in ipsilateral dorsal gray matter was diminished with complete and incomplete injuries; in the ventral regions, however, activity was increased with complete injuries, but with incomplete lesions, it was similar to or diminished compared with healthy subjects (i.e., it was notably less than in subjects with complete spinal cord injuries) [Stroman et al., 2004].
Serial MRI studies also can be helpful in following the evolution of traumatic spinal cord lesions [Sato et al., 1994; Sett and Crockard, 1991]. The need for metrizamide CT, used previously in evaluating post-traumatic spinal cord cysts and syringomyelia [Mace, 1985; Quencer et al., 1983; Rossier et al., 1983], has diminished substantially with the accuracy of MRI in showing these lesions. Also, because of the availability of MRI, the need for myelography to identify surgically remediable spinal cord injuries (e.g., extramedullary hematomas and major fracture-dislocations) has diminished greatly. When the patient’s clinical condition permits, most centers currently advocate early MRI for acute spinal trauma.
Electrophysiologic Evaluation
Motor-evoked potentials (MEPs) provide a means to assess descending spinal tract function. MEPs are induced by transcranial magnetic stimulation of the motor cortex and are recorded on muscles of interest using surface electrodes to determine the level and extent of the spinal cord injury. It has been shown that MEP amplitudes improve with spinal cord injury recovery but latencies do not [Xie and Boakye, 2008].
The usefulness of somatosensory-evoked potentials (SSEPs) and electromyography in evaluating the level of spinal cord injury and predicting clinical outcome is controversial. SSEPs are often useful in identifying the level of spinal cord injury [Louis et al., 1985] and in identifying areas of spinal cord damage that have been clinically unapparent [Toleikis and Sloan, 1987]. This test can be especially helpful in infants and young children in whom the degree of deficit often cannot be determined confidently by clinical examination [Kamimura et al., 1988]. It is unknown, however, whether SSEPs are superior to MRI in identifying the extent of a spinal cord injury and predicting clinical outcome. Some investigators have noted a high degree of correlation between abnormal SSEPs and potential for neurological recovery [Curt et al., 1997; Li et al., 1990; Perot, 1973; Rowed et al., 1976; Spiess et al., 2008; Ziganow, 1986], but others have not [Katz et al., 1991; York et al., 1983]. One study of experimental spinal cord injury revealed no correlation between the absence of SSEP waveforms and the degree of spinal cord injury [Singer et al., 1977]. In that study, animals demonstrated good return of function at 8–9 days, even though SSEP waveforms were not recordable 3–19 days after injury. Other studies have suggested, however, that patients with absent SSEPs after spinal cord injury are unlikely to have any meaningful recovery of neurologic function [Shurman et al., 1996].
The sympathetic skin response (SSR) is another noninvasive electrophysiological test, in which EMG electrodes placed on the skin surface record responses to electric or magnetic stimulation above the spinal lesion. These recordings can be used to assess damage to the spinal and peripheral efferent sympathetic pathways subserving corresponding skin areas. While SSR has been used less than MEPs and SSEPs to assess completeness of spinal cord injuries, the addition of sympathetic nervous system testing may provide a more complete picture of the spinal cord injury [Curt and Dietz, 1999; Xie and Boakye, 2008].
The presence of F-waves and H-reflexes depends on the integrity of the motor neuron pool. H-reflexes disappear in the first 24 hours of spinal shock, but return thereafter; F-waves disappear below the level of injury during spinal shock and reappear with its resolution [Horowitz and Patel, 2003]. F-wave and H-reflex latencies and electromyogram can show lower motor neuron unit abnormalities 3–4 myotome levels beyond the site of a spinal cord lesion [Shefner and Tun, 1991]. Based on such electrophysiologic findings, the extent of deficit, whether functional or anatomic, is often found to be more extensive than indicated by clinical examination. As with SSEPs, it is uncertain whether abnormalities on electromyogram can increase significantly the predictability of clinical outcome in spinal cord injury.
Clinical Syndromes
Intraspinal Intramedullary Injuries
Intraspinal intramedullary injuries can cause complete or incomplete loss of spinal cord function [Chilton and Dagi, 1985; Tator, 1983; Tator et al., 1993]. With complete loss, there is absence of all motor, sensory, and reflex function below the level of injury. With incomplete loss, some motor, sensory, and reflex function persists (see Box 78-1).
Complete Spinal Cord Injuries
Complete loss of spinal cord function, as defined by the ASIA/IMSOP Spinal Cord Impairment scale, can be either physiologic or pathologic. In physiologic loss, there is no morphologic alteration of the spinal cord, which becomes dysfunctional after impact. This dysfunction may occur with transient compression of the cord by a dislocated vertebra. With more sustained compression of the spinal cord, anatomic disruption of spinal cord elements may result, with accompanying pathologic loss of function. The frequency of complete spinal cord injury in pediatric patients varies widely, depending on the series reviewed, ranging from 20 to 95 percent of all pediatric spinal cord injuries [Anderson and Shutt, 1980; Burke, 1974].
The initial phase of complete loss of spinal cord function is characterized by spinal shock [Green and Eismont, 1984; Kiss and Tator, 1993]. The truncal and extremity muscles below the level of the lesion are flaccid, deep tendon and superficial reflexes are depressed or lost, plantar responses are absent, anesthesia is present to all modalities, and autonomic dysfunction (hypotension and bradycardia) is present. The mechanism of spinal shock is unknown, but its physiologic effects must be differentiated from the more permanent pathologic effects of spinal cord injury. Motor and sensory deficits resulting from spinal shock alone resolve within 1 hour. Persistence of motor and sensory deficits beyond 1 hour implies that pathologic, more permanent injury has occurred. After 6–13 weeks in adults and within 1 week in children, tendon reflexes return, and muscle tone improves. The reflexes later become pathologically active, and spasticity ensues if the injury is more permanent, and there usually is no significant return of motor or sensory function. A four-phase model of the sequential clinical changes seen in spinal shock and the neuronal mechanisms that may underlie those changes has been described:



 phase 4 (1–2 months), final hyperreflexia (from soma-supported synapse growth) [Ditunno et al., 2004].
phase 4 (1–2 months), final hyperreflexia (from soma-supported synapse growth) [Ditunno et al., 2004].After complete injury of the cervical or upper thoracic spinal cord, an acute syndrome of bradycardia, hypotension, and hypothermia can occur, probably because of disturbed sympathetic outflow at the cervical and upper thoracic levels; most patients with quadriplegia after spinal cord injury have chronic hypothermia with poor temperature control related to loss of sympathetic peripheral vascular control [Green and Eismont, 1984]. Recovery from complete spinal cord injury is rare. The prognosis is poor. Tator estimated that less than 2 percent of patients with complete injury recover some distal cord function [Tator, 1996]. More encouraging was a comprehensive review of several large series of patients with complete spinal cord injury, which found that about 2 percent of the patients became ambulatory [Hansebout, 1982].
Incomplete Spinal Cord Injuries
Cervical nerve root/brachial plexus neuropraxia
American football, a high-energy contact sport, places players at particularly high risk for cervical neuropraxic injuries. The relatively common “stinger” is a reversible peripheral injury resulting from neuropraxia of cervical nerve root(s) or brachial plexus, causing a temporary physiologic block in nerve conduction. It is characterized by unilateral burning pain radiating from the neck down the arm to the hand, usually lasting seconds to hours. There may be associated weakness of the deltoid and/or supraspinatus/infraspinatus muscles that resolves within 24 hours to 6 weeks. The most common mechanism of injury appears to be hyperextension, often with lateral flexion of the neck and an axial load, resulting in cervical nerve root compression caused by intervertebral foraminal narrowing. Additional mechanisms of injury are traction or stretching of the brachial plexus and direct trauma to the brachial plexus. Radiographs are usually normal. Cervical stenosis appears to be a predisposing cause [Rihn et al., 2009].
Cervical cord neuropraxia
Less common and more serious is cervical cord neuropraxia, due to hyperextension, hyperflexion, or axial loading of the cervical spine. Clinically, it is characterized by burning pain, paresthesias, and loss of sensation and/or weakness (ranging from no weakness to complete paralysis) in more than one limb, with rapid and complete resolution of symptoms within 10 minutes to 48 hours. Mechanically, the posterior-inferior margin of the vertebral body above and the anterior-superior portion of the lamina of the vertebra below combine to produce spinal cord compression (Penning’s pincer mechanism), with local anoxia and an increase in intracellular calcium temporarily disrupting spinal cord function. Radiographs often show congenital abnormalities, such as cervical stenosis and Klippel–Feil syndrome. Cervical cord neuropraxia occurs in 0.2 per 100,000 participants at the high-school level and 2 per 100,000 at the collegiate level [Rihn et al., 2009].

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


