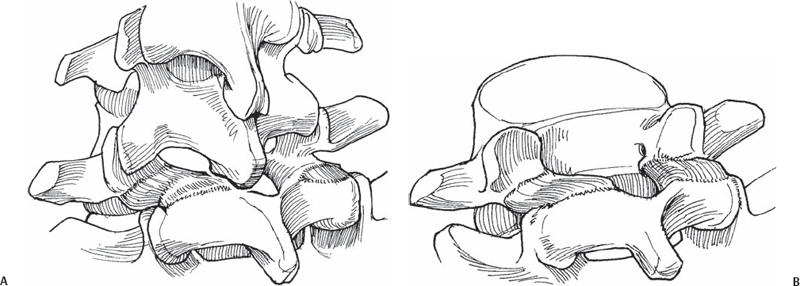
45 Christopher M. Bono Direct bone grafting and stabilization of spondylolytic (pars) lesions. Unhealed fractures of the pars interarticularis, also known as isthmic spondylolysis, can be chronically painful despite appropriate nonoperative treatments. Although patients with slippage (i.e., isthmic spondylolisthesis) are usually treated with fusion, direct repair of the nonunion without intersegmental lumbar fusion may be effective in some cases of spondylolysis without spondylolisthesis. Several techniques have been described, which generally involve bone grafting (usually autogenous) of the defect followed by some form of stabilization of the posterior elements. Methods of stabilization have varied from wire loop fixation, to interfragmentary compression screw, to pedicle screw-hook constructs. Though a clear clinical advantage of one technique over another has yet to be demonstrated, biomechanical studies suggest that a pedicle screw-hook construct offers the greatest stability at the nonunion site. As a basic tenet of nonunited fracture treatment, greater stability is usually desirable for better healing. To decrease low back pain from an unhealed spondylolytic (pars) defect by maintaining motion and avoiding intervertebral fusion. The patient is positioned prone on a radiolucent operating table. Using a lateral view, the proximal and distal extents of the incision are marked, with the former being the level of the cranial facet joint (usually L4-L5 for a planned L5 repair), and the latter being the superior aspect of the S1 lamina. In addition, a separate incision is marked over the iliac crest bone-graft harvest site. Alternatively, bone graft may be harvested through the same midline lumbar incision. It is important to understand the anatomy of the two fragments of the affected vertebra. The superior fragment consists of the superior articular processes, which are connected to the pedicles and transverse processes by a small portion of the pars (above the lesion). The proximal fragment is in continuity with the vertebral body. The distal fragment consists of the majority of the pars interarticularis (distal to the lesion), the laminae, the spinous process, and the distal articular processes. Adequately seating the hook at the lower border of the lamina.
Spondylolysis Repair (Pars Interarticularis Repair)
Description
Key Principles
Expectations
Indications
Contraindications
Relative
Absolute
Special Considerations
Special Instructions, Position, and Anesthesia
Tips, Pearls, and Lessons Learned
Difficulties Encountered
Key Procedural Steps
General Technique and Bone Grafting
Related posts:
 Lateral Extracavitary Approach
Open Reduction of Unilateral and Bilateral Facet Dislocations
Thoracoplasty: Anterior, Posterior
Thoracic Pedicle Screw Placement: Anatomic, Straightforward, and In-Out-In Techniques
Closed Cervical Traction Reduction Techniques
Rib Expansion Technique for Congenital Scoliosis
Lateral Extracavitary Approach
Open Reduction of Unilateral and Bilateral Facet Dislocations
Thoracoplasty: Anterior, Posterior
Thoracic Pedicle Screw Placement: Anatomic, Straightforward, and In-Out-In Techniques
Closed Cervical Traction Reduction Techniques
Rib Expansion Technique for Congenital Scoliosis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


