CHAPTER 199 Supratentorial Hemispheric Tumors
Hemispheric neoplasms account for 25% of all primary brain tumors in children beyond infancy.1 This chapter discusses supratentorial hemispheric tumors, which in the pediatric population are generally of a low-grade variety. Hemispheric tumors can be classified by cellular origin: glial, mixed glial and neuronal, and primitive neuroectodermal. Differentiation between these tumors can be accomplished with a careful history and examination and is often fairly apparent before biopsy or resection thanks largely to modern imaging technology. The therapeutic options, prognoses, and molecular genetics of these tumors are unique and frequently vary considerably from such lesions in adults.
Epidemiology
Supratentorial low- and high-grade gliomas each occur annually in less than 1 per 100,000 individuals younger than 20 years, with low-grade being more common.2 In total, glial tumors account for 56% of primary central nervous system (CNS) tumors in children younger than 14 years and for 45% of such tumors in those between the ages of 14 and 19.1 Supratentorial primitive neuroectodermal tumors (SPNETs) occur less frequently, with most children affected when younger than 10 years.3 There has been no demonstration of a higher predilection for gliomas or SPNETs between the sexes. Dysembryoplastic neuroectodermal tumors (DNETs), pleomorphic xanthoastrocytoma (PXA), and low-grade glioneuronal tumors are found in children more so than adults. Oligodendrogliomas and DNETs may occur slightly more frequently in males.4 Oligodendrogliomas are rarer in children than adults and account for less than 1% to 2% of primary pediatric brain tumors.1,5 PXA is less common still.6,7
Familial genetic syndromes increasing the likelihood for the development of primary intracranial tumors include Turcot’s syndrome (colonic polyposis), Li-Fraumeni syndrome, and neurofibromatosis type 1. A history of previous CNS tumor, systemic cancer, or cranial irradiation also increases risk for the development of secondary brain tumors, most notably meningiomas and high-grade gliomas.8 Of note, secondary high-grade gliomas are more commonly supratentorial and may exhibit a distinct genetic profile from their primary counterparts. Once diagnosed, secondary high-grade glioma portends a worse prognosis than primary tumors despite aggressive intervention. The St. Jude’s experience found a cumulative 4% 15-year risk for secondary neoplasms developing after treatment of a primary CNS tumor,9 and in children treated for acute lymphoblastic leukemia, there is a 1.39% cumulative incidence of secondary brain tumors (gliomas and meningiomas) at 20 years, with cranial irradiation being a dose-dependent predisposing factor.
Clinical Findings
Seizures are a frequent symptom of supratentorial lesions in children, particularly low-grade tumors such as fibrillary astrocytoma, PXA, DNET, and ganglioglioma.4,10,11 The likelihood for these tumors to be accompanied by seizures increases with their predilection to occur in the temporal lobe. However, some evidence exists to support the notion that neuronal elements of the tumor itself can act as independent generators of seizures,12 and secondary seizure foci may exist around the tumor.
Glial Tumors
Imaging
The majority of primary supratentorial hemispheric tumors in children are of glial origin. Imaging features that help in predicting the biologic behavior of hemispheric tumors in children include an imaging correlate of cellular density (density or intensity), the degree of mass effect, a cortical location, and any remodeling of the overlying calvaria. Standard evaluation of symptomatic children suspected of harboring an intracranial lesion typically begins with computed tomography (CT). Low-grade tumors are likely to appear hypodense, whereas high-grade gliomas are usually hyperdense. High-grade neoplasms are frequently associated with surrounding hypodense regions representing vasogenic edema. Non–contrast-enhanced CT is sensitive for regions of calcification, usually an indicator of a more indolent lesion, including ganglioglioma or oligodendroglioma.13 Remodeling of the inner table of the skull to conform to the gyral patterns or thinning is commonly seen with low-grade neoplasms. With the administration of intravenous contrast material, high-grade astrocytomas are expected to reveal enhancement attributed to regions of hypervascularity and breakdown of the blood-brain barrier (BBB). Cavitation surrounded by contrast heterogeneity is likely to represent necrotic components, a harbinger of a malignant phenotype. This cavitation is contrasted with the well-circumscribed ring of enhancement that surrounds benign cystic tumors.
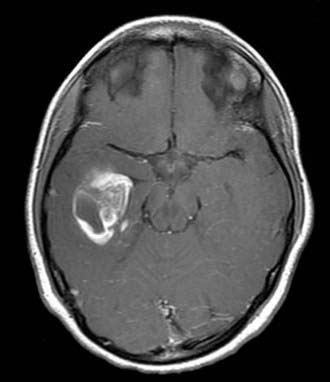
For enhanced anatomic definition and improved surgical planning, magnetic resonance imaging (MRI) has become the standard imaging modality. Low-grade fibrillary astrocytomas are frequently poorly delineated and will typically demonstrate gyral thickening, T1 hypointensity, and T2 hyperintensity, often best appreciated on T2 fluid-attenuated inversion recovery (FLAIR) sequences. PXA is more apt to show enhancing nodularity with frequent cystic components7 (Fig. 199-1).
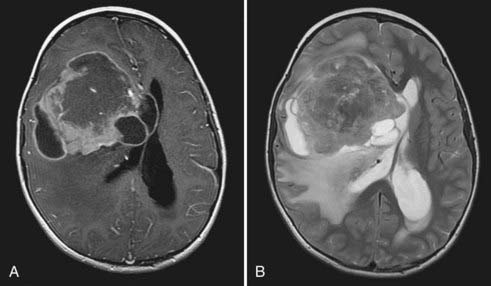
High-grade gliomas have mixed signal intensity, with predominant hypointensity on T1-weighted and hyperintensity on T2-weighted images.13 A broad region of T2 or FLAIR hyperintensity surrounding the tumor represents the highly infiltrative growth characteristic and surrounding edema frequently seen in these aggressive tumors (Fig. 199-2). This signal change most often extends in the direction of anisotropic white matter tracts and may cross the midline along commissural fibers, notably the corpus callosum. Regions of hypercellularity may result in restricted diffusion (bright appearance) within the lesion on diffusion-weighted imaging. Magnetic resonance spectroscopy, which is gaining popularity in narrowing the preoperative diagnosis of intracranial lesions, would be expected in high-grade components to demonstrate elevated peaks of choline, N-acetylaspartate, and lactate and a rise in the choline-to-creatine ratio.14
Pathology
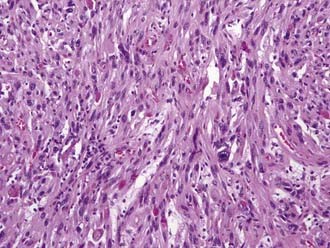
Classification or naming of these tumors is based on their cellular composition. Tumors composed of astrocytes with hypercellularity, infiltration, and a fibrillary matrix are designated fibrillary astrocytoma. The histologic hallmark of oligodendroglioma is perinuclear cytoplasmic shrinkage, which results in a halo appearance surrounding the cells’ nuclei and gives a classic “fried egg” appearance under lower magnification. The microvasculature takes on a “chicken wire” appearance, and calcifications may be seen grossly and under microscopy.15 PXAs have historically been thought to be purely astrocytic in origin, but these tumors may have neuronal progenitors as well. Histologically, these lesions show pleomorphism, lipid, reticulin, and perivascular lymphocytes (Fig. 199-3).
A critical distinction for the pathologist to make is between high- and low-grade lesions. Central review by an expert panel has been used in major studies to fulfill this task.16 Grade I astrocytoma, or juvenile pilocytic astrocytoma (JPA), is uncommonly hemispheric in location. High-grade or malignant gliomas represent World Health Organization (WHO) grades III and IV lesions. Grade III tumors demonstrate cellular pleomorphism, frequent mitoses, and the hypercellularity lacking in grade II lesions. Immunohistochemical testing will reveal positivity for glial fibrillary acidic protein (GFAP) and MIB-1 (anti–Ki-67 antibody). The most common grade III glial neoplasm is anaplastic astrocytoma (AA), but oligodendroglioma and PXA also have the potential to develop into grade III lesions.
The defining presence of necrosis raises the grade of the lesion to WHO IV and a diagnosis of glioblastoma multiforme. Pseudopalisading cellular architecture and significant microvascular proliferation are also seen. Like AA, immunohistochemistry is positive for GFAP. High-grade lesions will demonstrate a high mitotic index, and a high index of proliferation has been well characterized in Children’s Cancer Group (CCG) study 945 to correlate with worsened prognosis.17–19
Treatment
Unlike adult high-grade glioma, this diagnosis in children portends a 5-year survival rate of 30% to 50%, with a higher likelihood of long-term survivors.6,20,21 This prognosis is particularly significant and has relevance to survival from glioblastoma, where the mean survival of adults in contemporary series is less than 2 years.22 Cytoreduction on the order of 90% or greater has been associated with improved outcomes in children with high-grade glioma. The CCG studies 943 and 945 were instrumental in first demonstrating the value of total resection. Although it is difficult to control for adjuvant therapy, which varies from series to series, multiple reports have since corroborated a 5-year progression-free survival benefit of gross total resection on the order of greater than 20%. This holds true for both AA and glioblastoma.6,23–27 CCG 945 included 83 supratentorial high-grade gliomas for review and reported a 5-year progression-free survival rate of 35% for greater than 90% resection of glioblastoma versus 17% for subtotal resection. Furthermore, a 5-year progression-free survival rate of 44% was seen in children after total resection of AAs versus 22% for subtotal resection. These differences were statistically significant.27 The role of a second resection in improving survival for children with recurrent disease has yet to be well defined.
This goal of maximal tumor removal is also enhanced through the incorporation of several operative adjuncts. The principle of discriminating between tumor and parenchyma unifies all past and future improvements aimed at greater removal of tumor. The integration of high-resolution MRI with triplanar navigation is designed to offer the surgeon a reliable method for defining tumor margins with a greater degree of certainty. Errors attributed to brain shifting with partial tumor removal can be overcome with intraoperative modalities, including ultrasound and MRI. Tumor cell fluorescence may offer finer intraoperative resolution of tumor margins. Early results suggest that fluorescence-guided resection of glioblastoma in adults with the use of 5-aminolevulinic acid may improve the degree of tumor removal.28
For tumors associated with primary cortical regions, intraoperative brain mapping is an important safety mechanism. Motor function is assessed most reliably with this method, whereby direct cortical stimulation on the precentral gyrus triggers contralateral movement. The age of the child influences the ability to effectively perform cortical localization because of the variability in electrical impedance of the brain and the need for patient cooperation for language mapping. Older children will typically respond to a stimulus of 4 to 6 mA, whereas young children may require stimuli of 8 to 12 mA.29 Brain immaturity in children younger than 5 years may render direct stimulation ineffectual. In such cases, detection of the phase reversal potential between motor and sensory gyri is most likely to yield useful data. Because language mapping is reliant on intraoperative patient interaction and compliance, cortical localization of primary language representation is difficult in children younger than 10 years.30 Preoperative functional MRI has been shown to predict language dominance in infants and young children.31
Children with high-grade lesions or residual/recurrent low-grade gliomas may benefit from adjuvant radiation therapy. However, because of the well-established cognitive risks associated with cranial irradiation in very young children, radiation therapy is classically reserved for children older than 3 years.32 Cranial irradiation on the order of 50 to 60 Gy in children causes an average 10-point decline in IQ, with younger children being more adversely affected.33 Development of a secondary intracranial tumor is a significant risk in all children undergoing radiation therapy but is typically outweighed by the survival benefit in those with more aggressive malignancies. The risk of a secondary malignancy developing after radiation therapy has been reported to be just under 10%.34 With the development of conformal and fractionated therapy, delivery of radiation has progressed over time to allow higher doses to be given to the tumor while sparing surrounding normal brain.
The benefit of primary radiation therapy for low-grade glioma is dubious at best.16 Noteworthy studies evaluating adjuvant therapy for pediatric high-grade glioma, including the original CCG 943 publication in 1989, have included cranial irradiation as initial management in appropriate children.6,27,35 Most institutions currently use a fairly standard regimen of 50 to 60 Gy delivered to the tumor in roughly 25 fractions over a 5-week period for high-grade glioma. Data from recent studies suggest that the use of stereotactic radiosurgery, whereby a single high dose of radiation is delivered via intersecting beams to a desired tumor volume designated on a radiograph, should be reserved for patients with multiply recurrent low- and high-grade lesions who are not candidates for surgery.36–38
Chemotherapy is a vital component of multimodal treatment of high-grade glioma. The CCG 943 publication in 1989 established the use of chemotherapy as a standard initial adjuvant for pediatric high-grade glioma. That study prospectively randomized 58 children with high-grade glioma, 40 of whom harbored glioblastoma, into two therapeutic arms.25 One group underwent postoperative radiation therapy and combination chemotherapy consisting of lomustine, vincristine, and prednisone, whereas the other group underwent radiation therapy alone. The survival benefit in the chemotherapy group was significant, with a 5-year event-free survival rate of 46% versus 18% for radiation therapy alone.
The next most significant set of results came from CCG 945. Here, an “8 in 1” regimen of chemotherapeutics was administered to an experimental arm, whereas the control arm underwent the chemoradiation protocol in CCG 943. The “8-in-1” regimen consisted of vincristine, carmustine, procarbazine, hydroxyurea, dacarbazine, methylprednisolone, cisplatin, and cytarabine usually given in two cycles before radiation therapy and for up to 1 year afterward. Five-year event-free survival rates were higher in the “8-in-1” than in the standard therapy group (33% versus 26%).21
Oligodendroglioma, especially when anaplastic in nature, is also a good candidate for adjuvant therapy. Procarbazine, lomustine, and vincristine have been evaluated prospectively and been found to improve progression-free survival by almost 1 year in adults when administered in conjunction with surgery and radiation therapy.39,40 Overall survival is also improved in tumors harboring 1p and 19q loss of heterozygosity.
Chemotherapy is an even more important tool for children too young to undergo irradiation. For high-grade glioma, the North American Pediatric Oncology Group found a 3-year event-free survival rate of 43% for paired cyclophosphamide and vincristine and then cisplatin and etoposide without cranial irradiation.23,41 More recently, the French BBSFOP protocol demonstrated a 35% 5-year progression-free survival rate for surgical resection and chemotherapy alone.24 Despite being safer in long-term measures than radiation therapy for young children, the potential for toxicity, myelosuppression, and clinically significant infection is noteworthy and must be considered in patients with poor performance status.
With the addition in recent years of temozolomide to the armamentarium, the standards of treatment in adult neuro-oncology have decidedly changed. However, this generally well tolerated oral DNA-methylating agent has yet to show similar activity against pediatric high-grade glioma. This may in part be attributable to the differential response of methylguanine methyltransferase or the mismatch repair system in children, both of which potentially confer resistance. The Children’s Oncology Group recently published a large series of children undergoing temozolomide therapy for recurrent CNS tumors, 23 of which were high-grade gliomas. One child with high-grade glioma showed a partial response.42 With mechanisms of resistance in mind, the Pediatric Brain Tumor Consortium has recently reported phase I results for temozolomide given with the methylguanine methyltransferase inactivator O6-benzylguanine for recurrent high-grade glioma. Only four of eight patients completed therapy, but three did show a partial radiographic response to treatment.43
When high-grade gliomas arise as secondary tumors after treatment of a previous malignancy, the results are even more dismal. Responses to radiation therapy and chemotherapy are blunted, perhaps as a result of previous administration, and survival averages less than 1 year from the time of diagnosis.44






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


