Chapter 77 Surgical Management of Midbasilar and Lower Basilar Aneurysms
Epidemiology
In most neurosurgical series, aneurysms of the midbasilar and lower basilar artery represent less than 1% of cerebral aneurysms. Yamaura1 reported a frequency of 10 midbasilar and lower basilar artery aneurysms in 202 posterior circulation aneurysms (5%), whereas Sano and colleagues2 reported that they accounted for 7 of 1480 (0.5%) total cerebral aneurysms and for 7 of 116 (6%) posterior circulation aneurysms. In their earlier work, Peerless and Drake3 reported that midbasilar and lower basilar artery aneurysms accounted for 193 of all 1266 (15.2%) of their cases of posterior circulation aneurysms. In their more recent publication describing 1767 patients, aneurysms of the basilar trunk and vertebrobasilar junction were seen in 14.7% of patients.4
Recent large multicenter studies may overestimate the frequency of aneurysms in this anatomic location. In the original report from the International Study of Unruptured Intracranial Aneurysms, posterior circulation aneurysms (excluding basilar tip aneurysms) were seen in 6.2% of all patients.5 In a subsequent report from this study, these lesions composed 5.1% of all patients with unruptured aneurysms, 3.9% of which were clipped surgically and 8.9% of which were treated with endovascular coiling.6 Alternatively, the International Subarachnoid Aneurysm Trial probably incorporated a pre-established treatment bias in Europe, since only 2.7% of randomized patients had posterior circulation aneurysms and only one of the 2143 patients (0.05%) analyzed had a basilar trunk aneurysm.7
Principles of Management
Patients presenting with SAH and aneurysms located on the midbasilar and lower basilar artery are managed utilizing the same protocols previously established for other patients with SAH8: cardiorespiratory and basic neurologic supportive care, early ventriculostomy with cerebrospinal fluid (CSF) drainage in patients with Hunt-Hess8 grade IV or V SAH,9 early surgery in suitable cases,9–11 prophylaxis, and, when appropriate, aggressive management of post SAH cerebral vasospasm associated with ischemic deficit10,12,13 and aggressive management of increased intracranial pressure.9,10 Patients with neurologic symptoms related to mass effect of the aneurysm are managed semiurgently. Typically, these patients present with signs of brain stem compression or cranial nerve deficits, and careful consideration of their deficits is required during planning of the treatment approach and of the timing of intervention.
Endovascular management of aneurysms of the middle and lower basilar artery is increasingly reported.14–23 Although evidence of durability of treatment is still lacking, several recent reports have also described enhancements in surgical technique and outcomes associated with these improvements.24–32 Notably, the Pipeline embolization device (Chestnut Medical Technologies, Menlo Park, CA) is a self-expanding, microcatheter-delivered, cylindrical mesh device composed of braided cobalt, chromium, and platinum strands.19 The device, while not yet approved by the U.S. Food and Drug Administration (FDA), has a 30% to 35% metal surface area when fully deployed. Multiple devices can be deployed within each other (telescoped) to create a composite endovascular construct. The degree of metal surface area coverage can be manipulated by varying the technique of device deployment as well as by judiciously choosing the number of devices placed in a particular vascular segment. Evidence of its applicability for large midbasilar and lower basilar artery aneurysms is slowly becoming available—the device can be applied strategically to create an endovascular construct within a parent vessel that is rich with eloquent perforators.19,20 However, the Pipeline device has not yet been approved by the FDA.
The general rules for the anesthetic management of patients undergoing surgical clipping involve the use of preoperative corticosteroids and prophylactic intravenous antibiotics. Intraoperative hypotension is prevented, and intraoperative blood pressure is allowed to run mildly hypertensive, especially during any temporary vessel clipping. During exposure and clipping of the aneurysm, all patients receive intravenous doses of a barbiturate (thiopental) titrated to achieve electroencephalographic (EEG) burst suppression.
Hypothermic Cardiac Standstill
In certain cases, the size of the aneurysm precludes adequate visualization of the parent vessel and perforators. This problem is often most difficult with basilar artery aneurysms. In such situations, additional exposure can be obtained through the use of hypothermic cardiac arrest with barbiturate cerebral protection.33 During cardiac arrest, the aneurysm can be collapsed and the anatomic characteristics defined without the risk of hemorrhage. Since the original report from the Barrow Neurological Institute (BNI) in 1986,33 hypothermic cardiac arrest has been used in many patients with posterior circulation aneurysms.
The successful use of hypothermic cardiac standstill requires an experienced cardiovascular and cerebrovascular team. The success of hypothermic cardiac arrest for clipping complex aneurysms is partially determined by four key variables: depth of hypothermia, duration of circulatory arrest, use of barbiturates, and hemostasis.25 In the original BNI series, the mean brain temperature during standstill was 54°F, and the mean duration of standstill about 22 minutes (range, 3–72 minutes). The absolute maximum safe period of cerebral ischemia is unknown. The duration of cerebral ischemia that can be safely tolerated is significantly increased, however, by the utilization of profound hypothermia and precooling intravenous barbiturates administered to achieve burst suppression of EEG activity.
Anatomic Issues in Surgical Exposure
Previously, aneurysms at this location were treated through a subtemporal-transtentorial approach or a suboccipital approach.2,34–36 Although a transoral transclival or transmaxillary transclival approach has been used to expose the basilar artery by Peerless and Drake3 and others,2,37,38 they are associated with notable technical limitations of exposure and a significant risk of postoperative CSF leakage and meningitis.3 These various techniques can provide access, but they do not meet the requirements of maximal exposure combined with minimal brain retraction. A number of techniques have been devised to maximize lateral bone removal and to provide a relatively short and flat route of access to the front of the brain stem and the basilar artery: the transpetrosal approach,39,40 combined supratentorial-infratentorial approach,41 far-lateral approach,42–44 and far-lateral combined supratentorial-infratentorial approach.39 Each of these techniques, when appropriately matched to the location and size of the aneurysm, can provide excellent access to almost any aneurysm located on the midbasilar and lower basilar artery (Table 77-1).
Table 77-1 Surgical Approaches to Midbasilar and Lower Basilar Artery
| Transpetrosal Approaches |
| Retrolabyrinthine |
| Translabyrinthine |
| Transcochlear |
| Combined Supra- and Infra-Tentorial Approaches |
| Retrolabyrinthine |
| Translabyrinthine |
| Transcochlear |
| Far-Lateral Approach |
| Extreme Lateral Craniocervical Approach |
| Far Lateral: Combined Supra- and Infra-Tentorial (“Combined-Combined”) Approaches |
| Retrolabyrinthine |
| Translabyrinthine |
| Transcochlear |
| Anterior Transclival Approaches |
| Transoral (transpalatal) |
| Transmaxillary |
| Transfacial |
| Other Approaches |
| Extended orbitozygomatic |
| Anterior petrosectomy |
| Subtemporal |
| Unilateral suboccipital |
Transpetrosal Approaches
The anterior brain stem and clival regions can be reached through removal of portions of the petrosal bone with almost no brain or brain stem retraction.45 There are three variations of the temporal (petrous) bone dissection. The retrolabyrinthine technique involves petrous bone resection and preserves hearing. The translabyrinthine technique increases the amount of petrous bone resected and sacrifices hearing. Finally, the transcochlear technique involves maximal petrous bone resection, sacrifices hearing, and requires transposition of the facial nerve.41 Moving through these three variations represents a gradual increase in the amount of petrous bone resected and in the exposure of the brain stem and clivus.
Retrolabyrinthine Approach
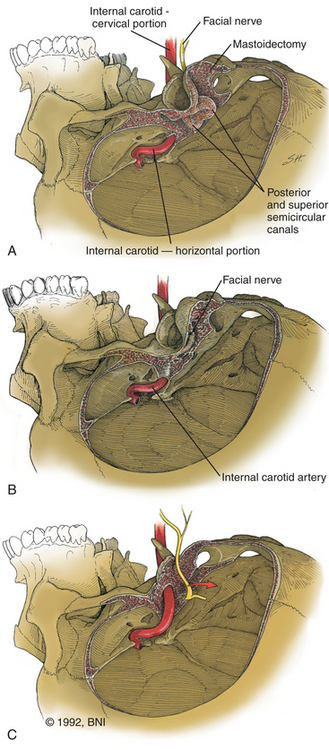
The retrolabyrinthine approach provides excellent access into the cerebellopontine angle but does not allow significant anterior visualization of the brain stem; therefore, it has a limited, isolated role in management of aneurysms of the midbasilar and lower basilar artery. If hearing is to be preserved, a retrolabyrinthine approach is used. The posterior and superior semicircular canals are skeletonized by drilling as far anteriorly as possible, both above and below the otic capsule, to expose as much dura as possible (Fig. 77-1A). The bone overlying the superior petrosal sinus and sigmoid sinus is removed with the drill. The endolymphatic sac and duct are preserved.
Recent studies describe a variation of the retrolabyrinthine approach designed to improve the surgical corridor to the midbasilar region but without necessarily jeopardizing hearing.28,30 Incidental or accidental injuries to the semicircular canals are not universally associated with hearing loss. Consequently, the transmastoid partial labyrinthectomy has been described as a modification of the standard retrolabyrinthine approach. The posterior and superior semicircular canals are occluded and resected, but the vestibule and lateral semicircular canal are preserved. Serviceable hearing can be preserved in 80% of patients using this technique.28
Translabyrinthine Approach
If greater exposure is required, the standard translabyrinthine approach, which sacrifices hearing, can be used. The initial part of this approach is performed as described for the retrolabyrinthine approach but involves the additional complete removal of all three semicircular canals and skeletonization of the posterior half of the internal auditory canal (Fig. 77-1B). More bone is removed from the face of the petrous pyramid than is possible through the retrolabyrinthine technique. Removal of all bone overlying the sigmoid sinus and, if necessary, the jugular bulb provides greater exposure of the inferior aspect of the clivus. The posterior external auditory canal and the bone overlying the mastoid segment of the facial nerve should also be thinned to minimize the obstruction to visualization of the clivus. The distal end of the superior vestibular nerve in the vestibule is used as a reference for identification of the facial nerve as it exits the internal auditory canal. The bone overlying the labyrinthine segment of the facial nerve is also thinned with cautious drilling utilizing a diamond bit and continuous intraoperative monitoring of facial nerve function.
Transcochlear Technique
For the greatest exposure of the clivus, the transcochlear technique is used (Fig. 77-1C). The external auditory canal is transected and oversewn in two layers. After the translabyrinthine exposure, the facial nerve is removed from its temporal bone canal,46 the greater superficial petrosal nerve is sectioned, and the facial nerve is transposed posteriorly, utilizing the dura of the internal auditory canal to protect part of the nerve. The entire tympanic portion of the temporal bone is removed with exposure of the periosteum of the temporomandibular joint. The internal auditory canal and cochlea are then removed. The jugular bulb is exposed by removal of the bone that separates it from the internal carotid artery at the skull base. The bone surrounding the carotid artery is removed to the siphon.
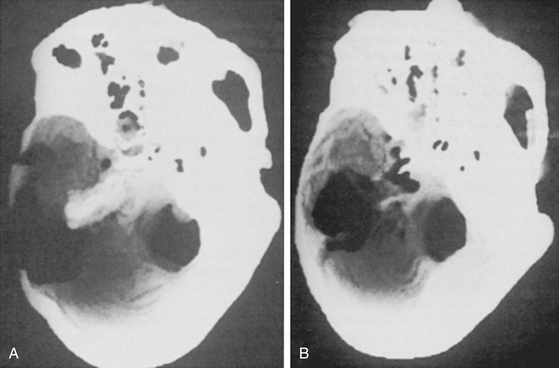
If direct exposure of the internal carotid artery is unnecessary, a thin rim of bone can be left encasing the vessel. The option of extensive internal carotid artery exposure allows creation of a direct saphenous vein bypass graft from the petrous portion of the internal carotid artery to the subarachnoid internal carotid artery if necessary.39,47 Bone is also removed from the floor of the plate of the middle fossa to the horizontal segment of the internal carotid artery. The difference in the amount of resection of the petrous ridge between the retrolabyrinthine and the transcochlear approaches can be appreciated on postoperative computed tomographic (CT) reconstruction scans (Fig. 77-2).
Intradural Exposure and Closure
Regardless of which of the previous extradural bony exposures is used, the dura mater is incised just inferior and parallel to the superior petrosal sinus and just superior to the jugular bulb. These two dural incisions meet at the sinodural angle and the porus acusticus. The dura mater of the internal auditory canal is opened, and the cerebellopontine angle is entered. The surgical procedure then proceeds according to the specific principles of aneurysm surgery as discussed earlier. After the aneurysm has been obliterated, the surgical field is closed in anatomic layers when possible. The temporal and occipital dura is reapproximated with 4-0 braided nylon suture. Abdominal adipose tissue, temporalis muscle, and fibrin glue are used to obliterate the eustachian tube in the translabyrinthine transcochlear approaches and to fill the void created by the temporal bone resection. Temporary lumbar spinal drainage of CSF is used for 3 to 5 days to prevent CSF leakage through the wound.
Selection of Surgical Approach
The salient features of the various approaches can be summarized as follows:
• The retrolabyrinthine approach provides excellent exposure of the cerebellopontine angle but not of the anterior brain stem and preserves function of both hearing and the facial nerves.
• The translabyrinthine approach offers greater exposure of the cerebellopontine angle and significantly improves exposure of the anterolateral and anterior brain stem, but at the expense of hearing and with an increased risk of CSF leakage.
• The transcochlear technique achieves the maximal exposure possible but accomplishes it with not only the disadvantages associated with the translabyrinthine technique but also an increased risk of facial nerve paralysis.
Apart from the morbidity associated with bone removal, a problematic aspect of all the transpetrosal approaches is that the surgical corridor to the aneurysm is necessarily lateral to the lesion by the nature of the bony exposure. This geometry can increase the difficulty of clipping the aneurysm because the surgeon may need to explore around the dome of the aneurysm during dissection in preparation for clipping and also may need to manipulate the aneurysm to visualize the entire neck during clipping. The senior author (RFS) has explored the use of alternate approaches, specifically the extended orbitozygomatic approach for lesions involving the distal two-fifths of the basilar artery or the far-lateral approach for lesions of the proximal two fifths of the basilar artery and vertebrobasilar junction.26 These approaches leave only the truly midbasilar (i.e., middle one fifth of the basilar artery) for transpetrosal approaches. The advantage of these alternate strategies, with or without hypothermic cardiac arrest, is that they allow visualization along the axis of the basilar artery, with good exposure of the neck and perforating vessels, facilitating aneurysm obliteration with a straight clip.
Using this more selected approach led to good scores on the Glasgow Outcome Scale (GOS)48 in 75% of patients (GOS 4 and 5).26 Only 11% had permanent treatment-related neurologic deficits. There were four deaths but only one occurred in the perioperative period.
Combined Supra- and Infra-Tentorial Approaches
Variations of the combined approach have been described since the first report in 1905 by Borchardt. However, it was mostly abandoned, partially as a result of a high mortality rate and improvements in the suboccipital approach offered by Cushing and Dandy. In 1966 Hitselberger and House40 described a combined suboccipital-petrosal approach for the removal of large cerebellopontine angle tumors and discussed how the wide exposure obtained with this technique overcame the individual limitations of the suboccipital and translabyrinthine approaches for dealing with extensive lesions. Their technique extended the translabyrinthine approach beyond the sigmoid sinus into the suboccipital areas, to achieve a wide view of the cerebellopontine angle with minimal brain retraction, and allowed the sigmoid sinus to be mobilized or divided to improve the surgical exposure.
Malis49 popularized the idea of combining the subtemporal and posterior fossa (suboccipital) approaches to improve the surgical exposure when treating extensive lesions of the clivus or medial petrous region. In Malis’s version, the petrosal bone is not extensively drilled, and the superior anastomotic vein (vein of Labbé) is preserved by ligation of the transverse sinus between the entrance of the superior anastomotic vein posteriorly and the sigmoid sinus and superior petrosal sinus anteriorly. After the transverse sinus is divided, the tentorium is split along the petrosal apex with sparing of the superior petrosal sinus. Elevation of the tentorium, transverse sinus, temporal lobe, and superior anastomotic vein allows exposure of the clivus down to the foramen magnum.
Morrison and King50 also described a translabyrinthine transtemporal approach to provide extensive exposure by drilling the petrous bone from the cerebellopontine angle upward into the middle fossa. Exposure is increased by division of the superior petrosal sinus and tentorium. In 1977, Fisch51 described the infratemporal fossa approach for extensive tumors of the temporal bone and base of the skull. Fisch combined a partial posterior and inferior petrosectomy with a cervicofacial approach. This approach provided good exposure of the jugular foramen but frequently required permanent anterior displacement of the facial nerve, resection of the zygomatic arch and mandibular condyle, and complete obliteration of the pneumatic spaces of the temporal bone. House and Hitselberger52 modified the translabyrinthine approach by adding the transcochlear technique. Pellet and colleagues53 combined the infratemporal approach of Fisch51 and the transcochlear approach of House and Hitselberger52 to create the widened transcochlear approach. This approach utilizes a petrosectomy to connect the posterior fossa to the superior carotid region, allowing for the single-stage removal of lesions that extend from the infratemporal region to the posterior fossa. The basic principles for the combined approach had thus been defined: variable amounts of petrous bone dissection with a supratentorial-infratentorial craniotomy and division of the tentorium. An important variable in the combined approach concerns the significance and fate of both the dural sinuses (superior petrosal, sigmoid, or transverse sinus) and the superior anastomotic vein.
A number of authors have also presented their experiences using variations of the combined infratemporal and posterior fossa approach for removal of large lesions involving the clivus and medial petrous region.41,54–57 Some advocate preservation of the major dural sinus,56,57 and others, with appropriate consideration for patency of the opposite transverse sinus, commonly sacrifice the sigmoid41,54 or transverse sinus.49
Surgical Technique
The patient is positioned supine on the operating table with the head positioned parallel to the floor, inclined slightly downward, and fixed to the operating table in a Mayfield headrest. A soft roll is placed under the ipsilateral shoulder to give appropriate support. The skin incision begins at the level of the zygoma, 1 cm anterior to the ear, and continues in a gentle curving fashion around the ear to just below the mastoid tip. To obtain greater exposure, the posterior part of the incision can be extended farther posteriorly. To obtain an exposure that includes the foramen magnum, this combined approach can be combined with the far-lateral suboccipital approach (discussed later).39,42–44 The scalp flap is retracted inferiorly with fishhooks attached to a Leyla bar. This maneuver exposes the lateral aspect of the skull: the zygoma, lateral temporal bone, external auditory meatus, and mastoid region. The neuro-otologist performs the approach through the temporal (petrous) bone, after which the neurosurgeon performs a craniotomy with exposure of the remaining sigmoid sinus and transverse sinus, followed by the intradural part of the procedure.
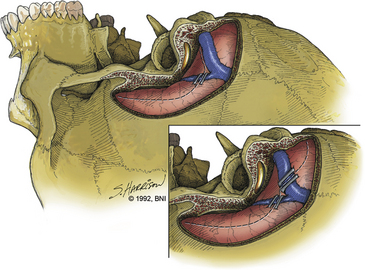
After the neuro-otologist has completed the petrous bone resection, the neurosurgeon proceeds with a subtemporal suboccipital craniotomy that crosses the transverse sinus and exposes the remainder of the sigmoid sinus. This craniotomy exposes a large dural surface. Brain relaxation, if required, is achieved initially with hyperventilation, administration of mannitol or barbiturates, or spinal drainage of CSF. Comprehensive electrophysiologic monitoring is routinely used: compressed spectral EEG, somatosensory-evoked potentials, brain stem auditory responses in both ears, or just the contralateral ear if ipsilateral hearing is to be sacrificed, and functional evaluation of facial and other appropriate cranial nerves. The anterior part of the dural incision (Fig. 77-3) is made over the temporal lobe and extends posteriorly to at least 1 cm below the site where the superior petrosal sinus enters the sigmoid sinus. Uncommonly, a low-lying superior anastomotic vein is found attached to the temporal dura or tentorium, and care must be exercised to prevent damaging this important vascular structure. If the sigmoid sinus is to be preserved, the dural incision crosses the superior petrosal sinus to join with a dural incision in front of the sigmoid sinus. The superior petrosal sinus can usually be cauterized or clipped and subsequently divided. Another incision can be made behind the sigmoid sinus (Fig. 77-3, inset)56 to allow access, if necessary, in front of and behind the sinus.
< div class='tao-gold-member'>
Related posts:
 Cortical and Subcortical Brain Mapping
Cortical and Subcortical Brain Mapping
 Radiation Therapy and Radiosurgery in the Management of Craniopharyngiomas
Radiation Therapy and Radiosurgery in the Management of Craniopharyngiomas
 Surgical Management of Intracerebral Hemorrhage
Surgical Management of Intracerebral Hemorrhage
 Neurovascular Decompression in Cranial Nerves V, VII, IX, and X
Neurovascular Decompression in Cranial Nerves V, VII, IX, and X
 Tumors Involving the Cavernous Sinus
Tumors Involving the Cavernous Sinus
 Arachnoid, Suprasellar, and Rathke’s Cleft Cysts
Arachnoid, Suprasellar, and Rathke’s Cleft Cysts
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


