Chapter 72 Surgical Treatment of Paraclinoid Aneurysms
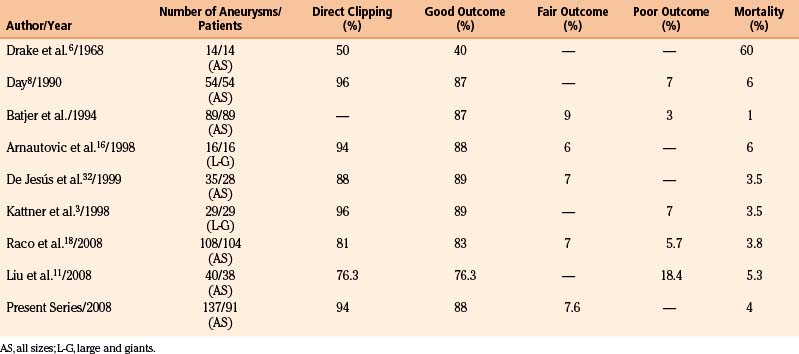
The portion of the proximal intradural internal carotid artery (ICA) adjacent to the anterior clinoid process (ACP) is called the paraclinoid segment. Aneurysms arising from the ICA between the roof of the cavernous sinus and the origin of the posterior communicating artery (PComA) are defined as paraclinoid aneurysms.1–5 These aneurysms are of considerable surgical interest due to their particular anatomic features and technical difficulties. Some of these aneurysms were considered in the past as unclippable or associated with very bad results when surgically approached.6 Fortunately, with the progressive refinement of microsurgical techniques their management has changed from the very conservative surgery to direct neck clipping, with results surpassing those of the endovascular therapy in terms of total neck obliteration and long-term recanalization (Table 72-1).4,5,7 The classification of these aneurysms according to the origin of their necks and projection of the aneurysms is particularly important to select the optimum microsurgical approach.1,8–12
Anatomic Aspects
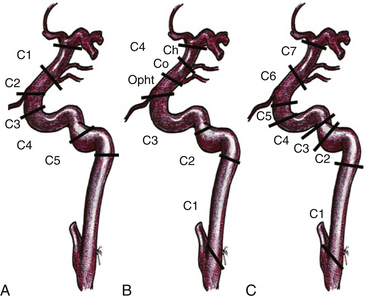
In 1938, Fisher12a published an anatomic nomenclature for the ICA based on the angiographic course of the artery, describing five segments designated C1 through C5. However, these segments were numbered opposite to the direction of blood flow and the extracranial ICA was excluded (Fig. 72-1A). Recently, other classifications have been published that include the extracranial and intracranial segments, and the carotid segments have been numbered according to the direction of the blood flow. Therefore, the paraclinoid segment of the ICA comprises the C2 and C3 segments of the original Fisher classification (1938), the distal C3 and Proximal C4 segment of Gibo et al. (1981),13 and the C5 and C6 segment of the Bouthillier classification (1996)14 (Fig. 72-1). Because of the close topographical vicinity of these aneurysms to osseous, fibrous, nervous and vascular structures of the skull base they may present with clinical symptoms due to compression of the optic nerve or other surrounding structures instead of the classic subarachnoid hemorrhage frequently seen in aneurysms in other locations.3,15 The anatomic structures of the paraclinoid area not only produce a limited space for expanding vascular lesions, but also for the neurosurgeon during operation, thus, sufficient proximal control and minimal manipulation of the vascular and nerve structures around are of utmost importance for the postoperative outcome.1,2,4,5,7,16–18
Classification
Given the variability in projection, size and origin of these aneurysms, various authors in the past have classified them. Most of the classifications are based on the site of origin of the neck, the projection of the dome and its relationship with branches arising from the ICA.2,7–10,12,17 The vast majority of saccular aneurysms arise within the angle formed by the parent artery and a significant arterial branch. Therefore, aneurysms related to these arteries are called accordingly, for example, ophthalmic and superior hypophyseal artery aneurysms.2,8 In addition, aneurysms unrelated to branches occur only rarely in this segment (distal ophthalmic aneurysms).12 Ventral paraclinoid carotid aneurysms seem to belong to the same category as infraophthalmic aneurysms, which originate from the ventral surface of the ICA and in which the proximal aspect of the neck is located approximately at the level of the ophthalmic artery and the distal aspect of the neck is located proximal to the posterior communicating artery19 (Fig. 72-2). These aneurysms also project straight or slightly medial and downward. Carotid cave aneurysms are another distinct type of aneurysm located at non-branching sites of this segment. This type of aneurysm arises from the medial wall of the proximal intradural ICA, and grows within a small dural recess, with the apex of the sac directed toward the cavernous sinus10 (Fig. 72-3). All these denominations have contributed to create a rather complex view of these aneurysms. Another confusing characteristic is that they are not always related to a branching artery and may point in any direction, as laterally, medially, ventrally, or dorsally (Fig. 72-2).
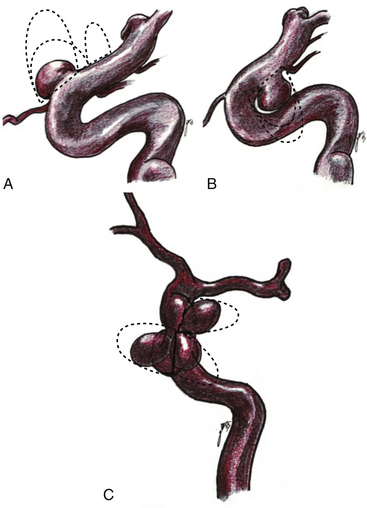
In order to simplify the classification of these aneurysms, we prefer to name them according to their site of origin in relation to the circumference of the ICA and some branching artery (if any), because this is also relevant at the time of clipping. Thus, the paraclinoid aneurysms can be classified as follows: dorsal type aneurysms, ventral type aneurysms, carotid cave aneurysms, and global type aneurysms (Figs. 72-3 to 72-7).
Dorsal Type Aneurysms
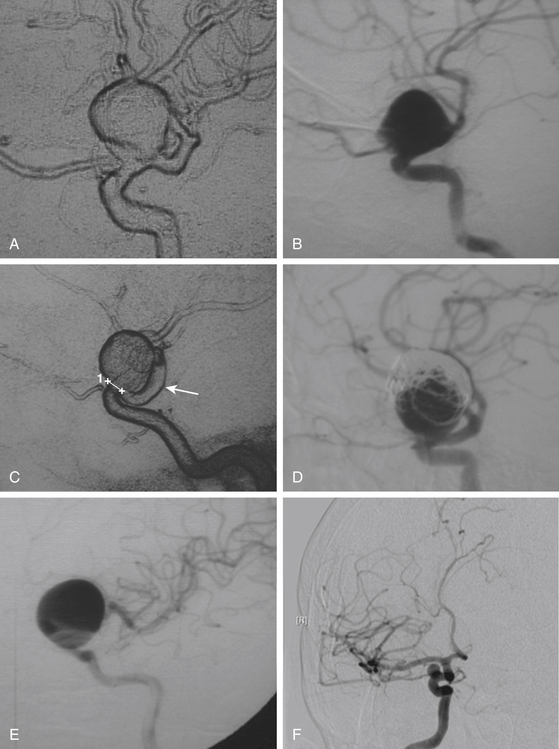
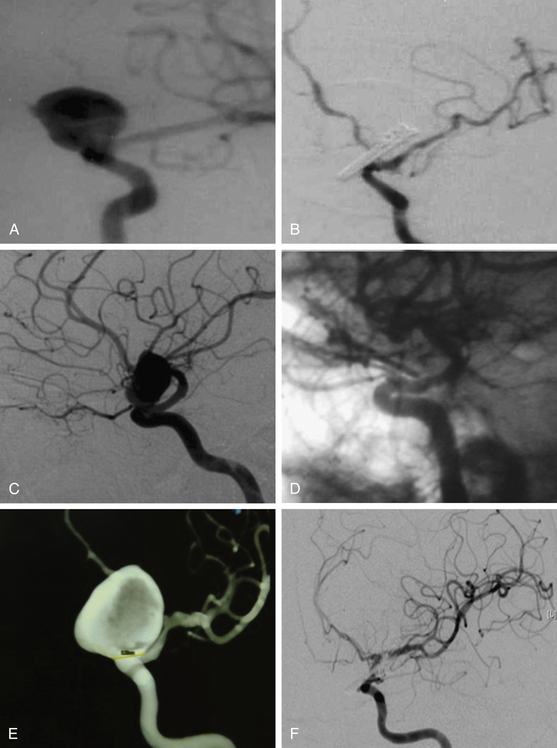
These include the proximal dorsal type aneurysms that correspond to the carotid ophthalmic aneurysms. They arise from the ophthalmic segment of the ICA in close relationship with the ophthalmic artery.7,9,11,15,18 On the lateral view of an angiogram the neck of the aneurysm is located just distal to the origin of this artery (Figs. 72-2A, 72-4, and 72-8). They grow upwards and cause compression of the optic nerve. As they have a tendency to grow, many of these lesions are detected because of visual deficits. The second main type is the distal dorsal type aneurysm (also known as dorsal wall aneurysms). This aneurysm grows upward at the dorsal surface of the ICA (Fig. 72-5). They are located distal to the ophthalmic artery and seem not to origin from any branch of the ICA.9,12 Whether they arise at bifurcations of vestigial arteries or because hemodynamic stress at the curvature of the carotid siphon is unknown.20 The dorsal surface of the ICA is also a common site of blood blister–like aneurysms. These are dangerous small lesions with fragile walls consisting of normal adventitia or fibrin nets. Primary treatment in the acute stage is challenging due to the substantial risk of intraoperative bleeding, resulting in the formation of a large defect in the ICA. To treat these aneurysms, sometimes it is necessary to use especially designed encircling clips or some wrapping procedure, otherwise, a bypass procedure with trapping of the aneurysm can be used as an alternative.
Ventral Type Aneurysms
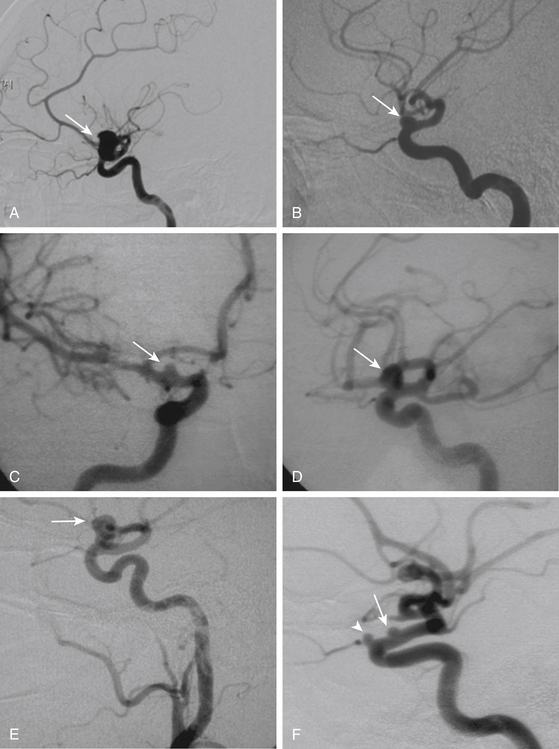
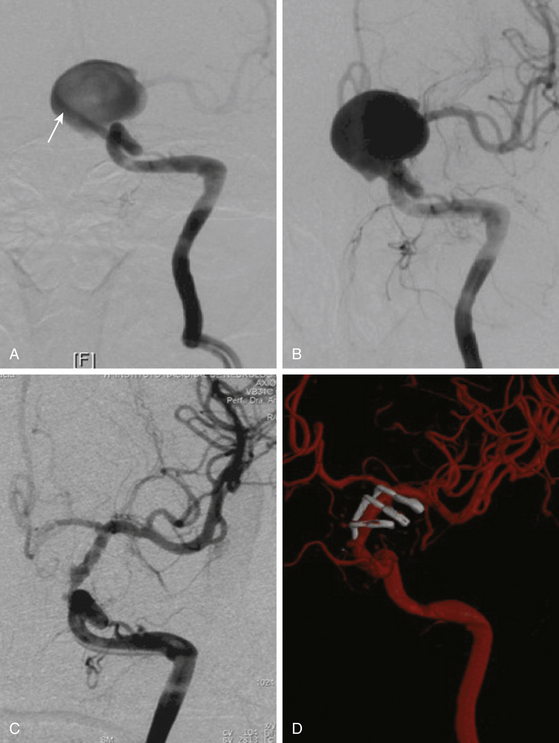
These aneurysms grow at the ventral or ventromedial surface of the ICA (Figs. 72-2B, 72-6, and 72-9). They are located opposite to the origin of the ophthalmic artery and in close relationship with the superior hypophyseal artery. As they increase in size, they are directed downward and medially. When large or giant, they produce an upward displacement of the ICA; however, visual disturbance is not as frequent as in dorsal type aneurysms.1,2,5,8,19
Carotid Cave Aneurysms
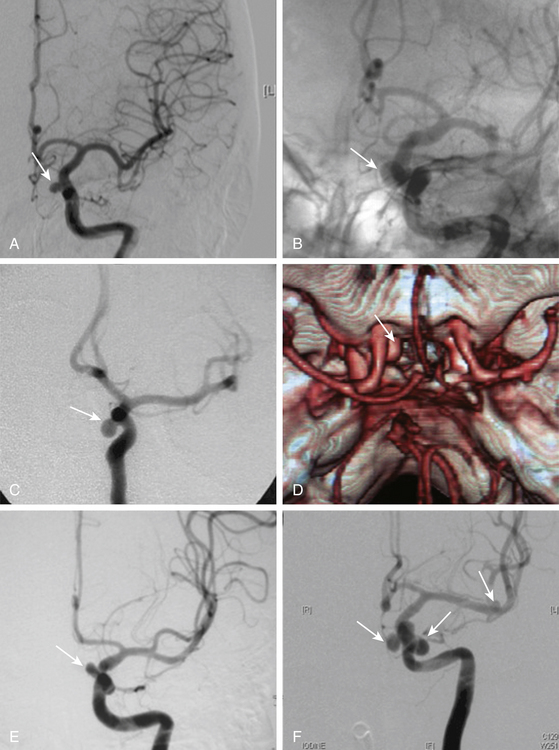
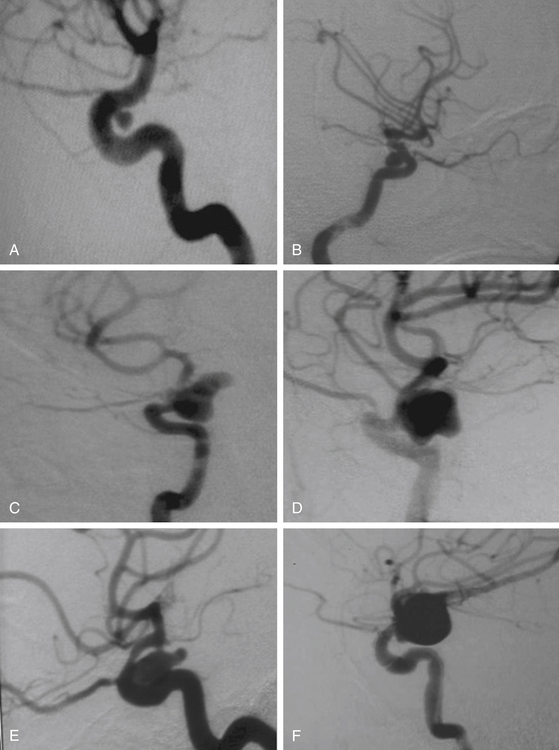
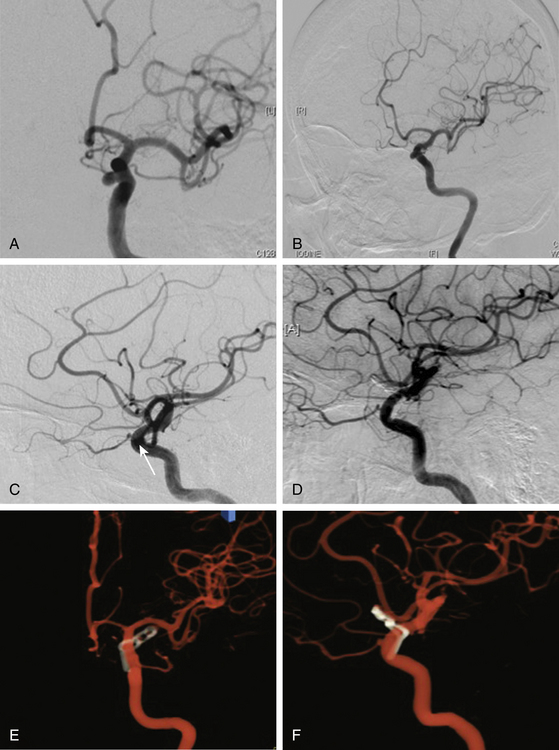
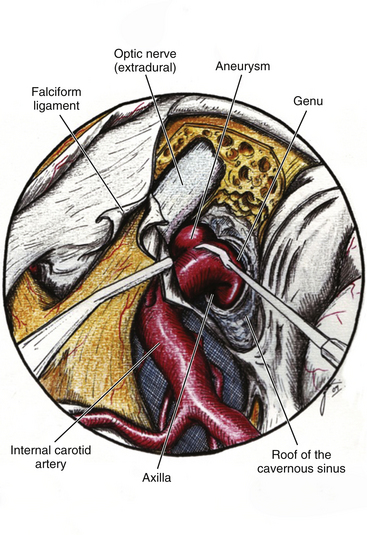
This is a special type of aneurysm originating between the proximal and distal carotid rings. They grow ventromedially proximal to the ophthalmic artery, and are visible mainly on the anterior or oblique angiographic views. On the lateral view, they remain hidden by the ICA (Figs. 72-3 and 72-10). Carotid cave aneurysms are transitional in type between paraclinoid intradural and cavernous sinus aneurysms. They may grow out of the cave into the intradural subarachnoid space. During surgery, they project ventrally at the level of the carotid genu10 (Fig. 72-11). In this sense, the surgical genu is located more proximal than the angiographic genu, which roughly corresponds to the location of the dural ring.
Global Type Aneurysms
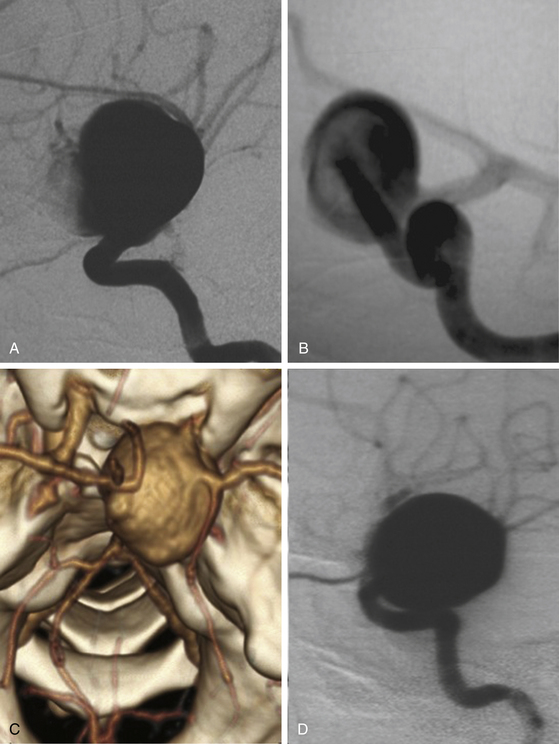
These aneurysms involve the entire circumference of the ICA; they are large or giant in size, and during angiography or surgery the origins of the neck are not as easy to identify as ventral or dorsal types even when the origin was surely at any of these points. Most cases are associated with degeneration of the carotid wall. The importance of this type of aneurysm is that the treatment is based on deconstructive techniques (parent artery obliteration and bypass surgery). This type of aneurysm should not be diagnosed only because of size and shape (Fig. 72-7).
It should be emphasized that during the growth process of a paraclinoid aneurysm, the dome could occupy anatomic spaces at the medial or lateral side of the ICA (Fig. 72-2). We do not believe that the medial or lateral sides of the ICA are origin sites of such aneurysms. When we carefully analyze the angiographic videos and films or the intraoperative recordings (except for global type aneurysms), the origin can be traced to the dorsal or ventromedial surface of the ICA.
Preoperative Planning
A very careful preoperative plan should be obtained for every case, taking into account the size and position of neck and dome of the aneurysm and its relationship with surrounding structures, especially the optic nerve. In addition, the length of the ICA should be assessed as well as the position of the ophthalmic and posterior communicating arteries. The summary of all this information will provide important hints for selecting the craniotomy and the technique for drilling the ACP (extra or intradural), and to prepare the availability of proper instruments to be used in the operation including a complete set of ring (fenestrated) clips for ventral or carotid cave aneurysms. To prevent premature intraoperative rupture or prolonged ICA occlusion, the preoperative angiography should include a four-vessel angiography with a balloon or manual compressive test occlusion in the awake patient. This will provide information about the position of the aneurysm and the collateral circulation at the circle of Willis, especially from one side to the other through the anterior communicating artery and from the posterior to the anterior circulation. The results of this preoperative test allow for reliable estimation of the tolerance of temporary or even permanent ICA occlusion or to be prepared for a bypass procedure before attacking a complex aneurysm in case of poor collateral circulation2,3,21 (Fig. 72-12).
< div class='tao-gold-member'>
Related posts:
 Chemotherapy for Brain Tumors
Current Surgical Management of High-Grade Gliomas
Endoscopic Endonasal Approach for Craniopharyngiomas
Revascularization Techniques in Pediatric Cerebrovascular Disorders
Surgical Management of Parasagittal and Convexity Meningiomas
Surgical Management of Major Skull Defects and Potential Complications
Chemotherapy for Brain Tumors
Current Surgical Management of High-Grade Gliomas
Endoscopic Endonasal Approach for Craniopharyngiomas
Revascularization Techniques in Pediatric Cerebrovascular Disorders
Surgical Management of Parasagittal and Convexity Meningiomas
Surgical Management of Major Skull Defects and Potential Complications
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


