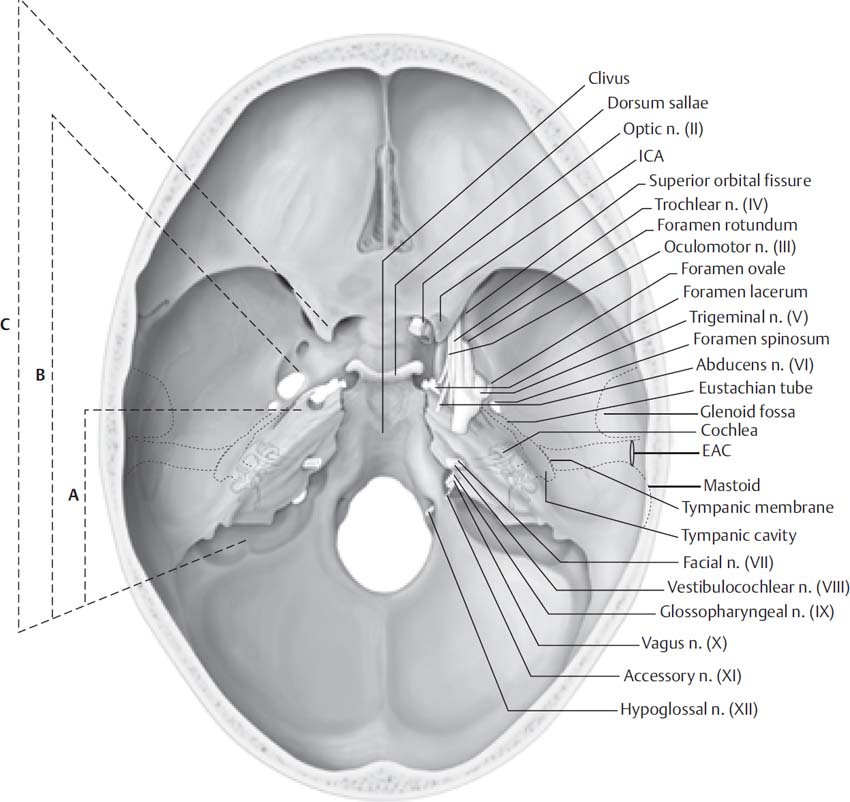
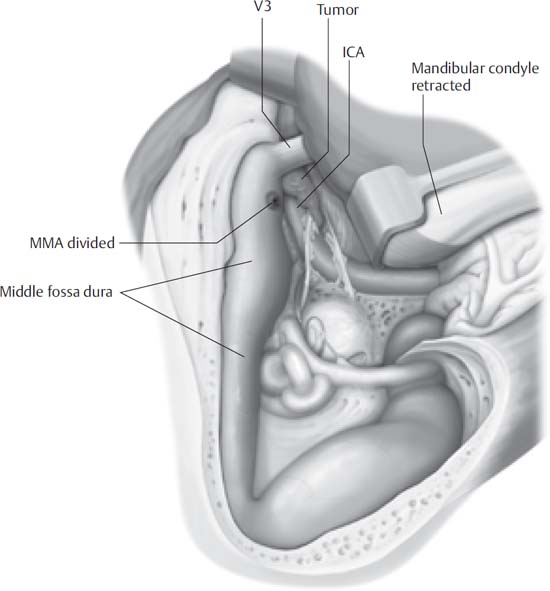
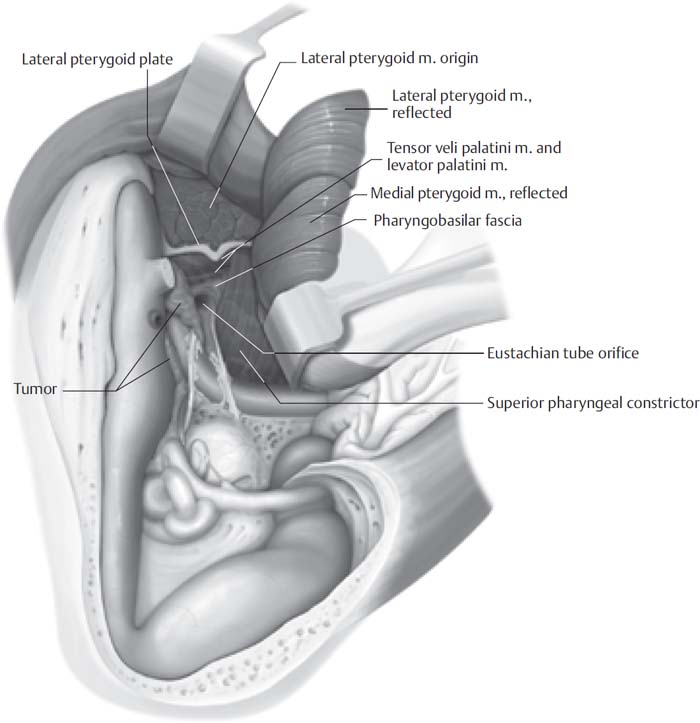
11 The infratemporal fossa is a well-guarded area of the skull base. The facial nerve and carotid artery are the main obstacles to accessing this region with minimal morbidity. Ugo Fisch developed a systematic approach to lesions of the infratemporal fossa in the 1970s. The type A approach, and modifications thereof, are utilized in accessing the jugular foramen and lesions medial to the facial nerve. As the type A approach is covered in Chapter 10, it will not be discussed further here. The type B approach allows access to the petrous apex, clivus, horizontal segment of the intratemporal carotid artery, and the posterior infratemporal fossa. Lesions anterior to the external auditory canal may be approached by leaving the facial nerve within the fallopian canal, thereby reducing the chance of paresis that may occur with the type A approach. The type C approach is an extension of the type B approach and allows access to the infratemporal fossa, pterygopalatine fossa, parasellar region, and the nasopharynx. The different exposures obtained with the Fisch types A, B, and C approaches are demonstrated in Fig. 11.1. Type B and C approaches provide exposure to benign lesions of the infratemporal fossa, petrous apex, and clivus. The decision to use these approaches in the treatment of malignancies involving the skull base should not be made lightly. Piecemeal removal of tumors should be expected. En bloc removal of tumors with adequate margins is usually not possible without producing significant morbidity. Figures 11.1, 11.2, and 11.3 schematically demonstrate the anatomic exposure obtained in the type B and C approaches. • Type B approach: benign lesions of the petrous apex, clivus, and posterior infratemporal fossa • Type C approach: skull base lesions involving the infratemporal fossa, the pterygopalatine fossa, the parasellar region, and the nasopharynx The infratemporal fossa provides the most challenging anatomy for the skull base surgeon. Mastering the anatomy of the infratemporal fossa requires a thorough understanding of the bony, muscular, and neurovascular contributions to this area. The bony anatomy of the infratemporal fossa is demonstrated in Figs. 11.4, 11.5, and 11.6. Note the linear relationship of the mastoid tip, stylomastoid foramen, sphenoid spine, foramen spinosum, foramen ovale, and the lateral pterygoid plate. The eustachian tube and carotid artery run parallel and medial to this line, with the carotid artery lying medial to the eustachian tube. Fig. 11.1 The Fisch-described infratemporal fossa approach has three variations providing a graded level of anterior and medial exposure. The type A provides exposure to the region of the jugular foramen, the vertical segment of the internal carotid artery (ICA), and the posterior infratemporal fossa. The type B provides additional exposure to the petrous apex and horizontal ICA and the clivus. The type C provides an extension to the anterior infratemporal fossa, the nasopharynx, the pterygopalatine fossa, and the cavernous sinus. Pertinent skull base anatomy as seen above is labeled. EAC, external auditory canal. The muscles of the infratemporal fossa include the medial and lateral pterygoid muscles and the temporalis muscle. The temporalis muscle originates on the lateral surface of the skull, the temporal fossa, and the posterior border of the frontal process of the zygomatic bone. The blood supply originates from the maxillary artery via the deep temporal arteries. These arteries lie on the deep surface of the temporalis muscle and may be injured during elevation of the muscle if not carefully preserved. The lateral pterygoid muscle originates on the greater wing of the sphenoid and lateral aspect of the lateral pterygoid plate to insert on the medial mandibular neck. The medial pterygoid originates on the medial side of the lateral pterygoid plate and follows an inferior course as it inserts on the medial mandibular neck. Fig. 11.2 Infratemporal fossa type B. The facial nerve is rerouted anteriorly, and the horizontal intrapetrous carotid artery is exposed to gain safe access to the petrous apex and clivus. This approach requires removal of the glenoid fossa, division of the middle meningeal artery (MMA), and division of V3. ICA, internal carotid artery. The maxillary artery arises from the external carotid artery and passes medial to the ramus of the mandible (mandibular portion of the maxillary artery) to enter the infratemporal fossa (Fig. 11.5). It may course medial or lateral to the inferior head of the lateral pterygoid. This pterygoid portion of the maxillary artery give rise to the middle meningeal, inferior alveolar, pterygoid, masseteric, and deep temporal arteries. The maxillary artery then enters its pterygopalatine portion after passing through the sphenopalatine fissure. Great care should be taken to preserve the deep temporal arteries, as they provide the primary blood supply to the temporalis muscle. An understanding of the fascial planes of the temporal region is also mandatory. There are three primary fascial layers within the temporal region that are of primary importance, particularly in their relationship to the facial nerve (Figs. 11.7 and 11.8). The temporoparietal fascia (superficial temporal fascia) is an extension of the superficial musculoaponeurotic system (SMAS) and is in continuity with the galea and frontalis muscle. This layer envelops the frontal branch of the facial nerve and the superficial temporal artery. The deep temporal fascia is composed of two layers: the superficial and deep layers. The superficial and deep layers of the deep temporal fascia split at the temporal line of fusion to envelop the zygomatic arch. The superficial temporal fat pad rests between these layers and extends down to the zygomatic arch. This fat pad provides an excellent landmark for the appropriate plane of dissection to access the zygoma and protect the frontal branch of the facial nerve. Fig. 11.3 Extension to the infratemporal type C approach. This allows access to the pterygopalatine fossa, the nasopharynx, and the cavernous sinus.
The Fisch Infratemporal Fossa Approach: Types B and C
 Indications
Indications
 Surgical Anatomy
Surgical Anatomy
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


The Fisch Infratemporal Fossa Approach: Types B and C
