4 Thoracic Spine
I. Key Points
– The normal thoracic spine includes 12 rib-bearing vertebral segments; anatomical variations can have 11 or 13 rib-bearing segments.
– Compared with the cervical and lumbar spine, the motion of the thoracic spine is limited due to the osteoligamentous relationship with the rib cage.
– Normal thoracic kyphosis is 10 to 40 degrees with the apex at T7.1
II. Bony Anatomy (Figs. 4.1 and 4.2)2
– The dorsal, ventral, and lateral diameters of the vertebral bodies increase from the upper to lower thoracic spine.3
– Thoracic kyphosis results from the wedge shape of the vertebral bodies, in which the anterior vertebral body height is less than the posterior vertebral body height.1,3
– The ribs from T2 to T9 articulate with two vertebral bodies (at the demifacets) and the transverse costal facet of the caudal vertebral body (i.e., T2 rib articulates with T1 and T2 at the demifacets and the T2 transverse facet).
– The T1, T11, and T12 (and often T10) ribs have a full facet for articulation with the corresponding vertebrae.
– The eleventh and twelfth ribs do not articulate with the transverse process of the corresponding vertebral body.
– The thoracic facets are oriented in an intermediate plane compared with the relatively coronally oriented cervical facets and the sagittally oriented lumbar facets, and provide stability in flexion and extension.1,3
– Sagittal pedicle height gradually increases from the upper to lower thoracic spine.3
– Transverse pedicle width decreases from the upper thoracic spine to the mid-thoracic spine (T5-T6) before gradually increasing through the lumbar spine.1,3
– The transverse pedicle angle decreases from T1 to T12.3
– The diameter of the spinal canal is smaller in the thoracic than in the cervical and lumbar regions.
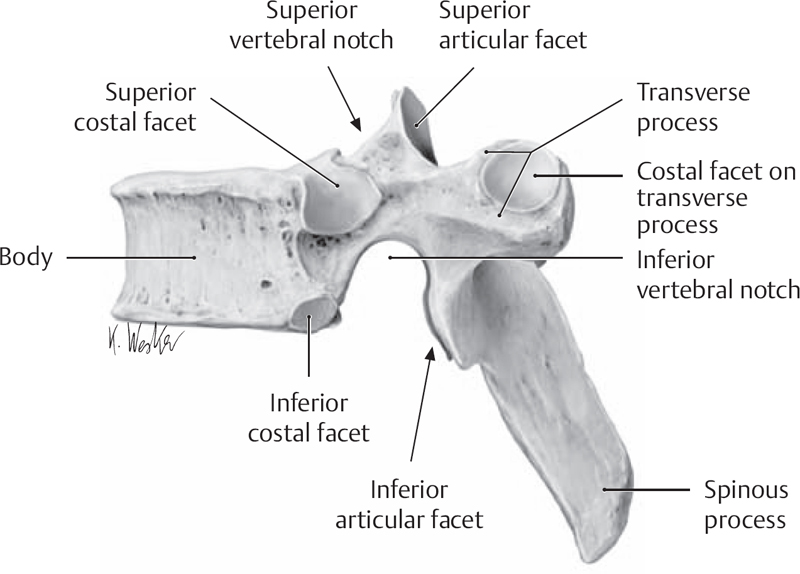
Fig. 4.1 Lateral view of thoracic vertebra (from THIEME Atlas of Anatomy, General Anatomy and Musculoskeletal System, (c) Thieme 2005, Illustration by Karl Wesker).
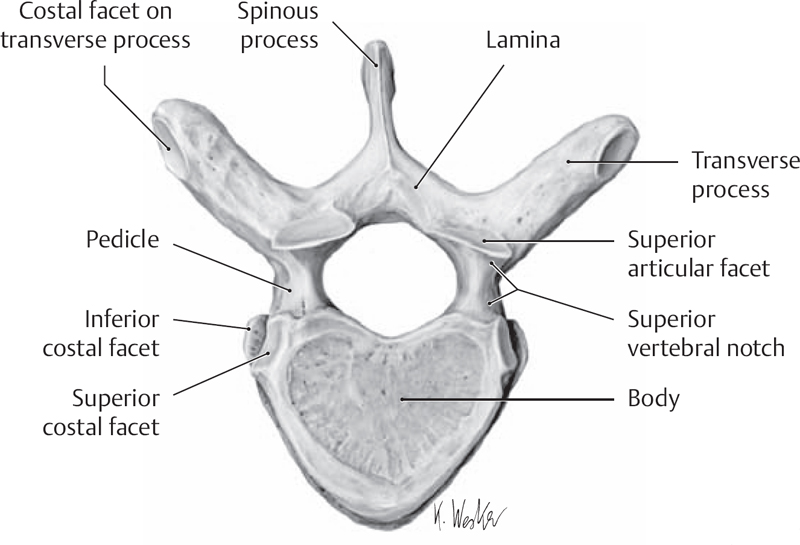
Fig. 4.2 Superior view of thoracic vertebra (from THIEME Atlas of Anatomy, General Anatomy and Musculoskeletal System, (c) Thieme 2005, Illustration by Karl Wesker).
III. Neural Anatomy
– The thoracic nerve roots exit below the pedicle of the corresponding vertebra (i.e., T3 nerve root exits below the T3 pedicle).
– Thoracic nerves supply the trunk and abdomen. Important thoracic dermatomes include T4 at the nipple line, T6 at the base of the sternum, and T10 at the umbilicus.
– The spinal cord runs through the length of the thoracic spinal canal and ends at the conus medullaris, usually at the L1-L2 level.
IV. Vascular Anatomy
– The anterior spinal artery arises from vertebral arteries and runs in the anterior median fissure of the spinal cord.
– The paired posterior spinal arteries usually arise from the posterior inferior cerebellar arteries and travel lateral to the posterior median sulcus of the spinal cord.
– Segmental arteries from the lumbar and intercostal arteries supplement the arterial supply of the cord through six to eight radicular arteries.
– The artery of Adamkiewicz is the largest radicular artery and provides the main arterial supply to the cord from approximately T8 to the conus. It arises from the T9-L2 region in 85% and from the left side in 80% of people.1,3
V. Ligamentous and Muscular Anatomy (Table 4.1)
– Muscles of the thoracic spine
• Deep layers
 Rotatores longus and brevis, levatores costarum longus and brevis, multifidus, semispinalis thoracis, and external costal muscles
Rotatores longus and brevis, levatores costarum longus and brevis, multifidus, semispinalis thoracis, and external costal muscles
• Intermediate layers
 Splenius cervicis, serratus posterior superior and inferior, and erector spinae: spinalis thoracis, longissimus, iliocostalis
Splenius cervicis, serratus posterior superior and inferior, and erector spinae: spinalis thoracis, longissimus, iliocostalis
• Superficial layers
 Rhomboid, latissimus dorsi, and trapezius
Rhomboid, latissimus dorsi, and trapezius
VI. Surgical Pearls
– Laminectomy of the thoracic spine can increase the risk of progressive kyphosis due to the loss of the posterior tension band.
– Injury to the artery of Adamkiewicz can cause a spinal cord infarction due to the tenuous blood supply of the lower thoracic cord.
– Due to variable thoracic pedicle anatomy, a thin-cut computed tomography (CT) scan can be useful prior to thoracic pedicle screw placement to assist with surgical planning and avoid neural injury.
– Avoid ending spinal constructs at the thoracic kyphotic apex to prevent early instrumentation failures.
Table 4.1 Principal Thoracic Ligaments: Their Attachments and Modes of Action
Common Clinical Questions
1. True or false: The pedicles on the concavity of a scoliotic curve tend to be larger than the pedicles on the convexity of the curve.
2. True or false: Each rib usually articulates only with its corresponding vertebral body.
3. The apex of normal kyphosis in the thoracic spine is at which level?
A. T2-T3
B. T5-T6
C. T7-T8
D. T9-T10
E. T11-T12
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


