In most common protocols, TMS is coupled with surface EMG (TMS-EMG) such that the motor cortex is stimulated and the magnitude of the evoked muscle contraction in a contralateral limb (typically a hand muscle) can be quantified by skin electrodes and the recording of a motor evoked potential (MEP) (reviewed in Ref.
2). From the MEP, a number of measures can be derived to probe cortico-spinal excitability (
Table 53.1) and a number of them characterize cortical and intracortical excitation/inhibition balance. One is the threshold to muscle activation or motor threshold (MT). The MT, obtained by single-pulse TMS, appears to reflect largely sodium channel-mediated membrane excitability in efferent pyramidal cells, and is increased by anticonvulsants, such as phenytoin and carbamazepine that inhibit voltage-gated sodium channels. Additionally, paired-pulse TMS (
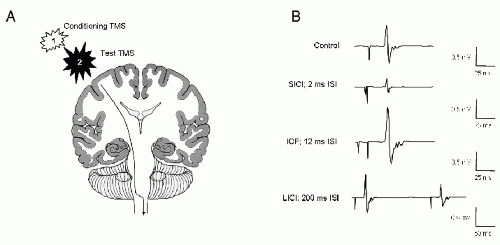
Fig. 53.1) provides measures of γ-aminobutyric acid (GABA)-mediated corticocortical inhibition and glutamate-dependent cortico-cortical excitability. In the most common paired-pulse TMS protocols, a subthreshold conditioning stimulus is delivered before each succeeding TMS pulse (reviewed in Refs.
2,
10). Short (1 to 5 msec) interstimulus intervals lead to reduction of the MEP, and likely reflect GABA
A receptor-mediated short-interval intracortical inhibition (SICI). Slightly longer (6 to 20 msec) interstimulus intervals augment the MEP, reflecting glutamatemediated intracortical facilitation (ICF). Benzodiazepine (GABA
A receptor agonist) anticonvulsants such as diazepam and lorazepam enhance SICI and suppress ICF (
11, reviewed in Ref.
12). Still longer interstimulus (50 to 300 msec) paired-pulse TMS-EMG protocols can also measure GABA
B receptor-mediated long-interval intracortical inhibition (LICI) that is enhanced by the GABA
B receptor agonist baclofen (
13,
14). The extent of cortical inhibition may also be measured by the cortical silent period (CSP), a transient EMG silence observed when TMS is delivered to the motor cortex during an active motor contraction. The CSP too appears mediated by GABA receptors, although the contributions of GABA
A and GABA
B receptors to CSP is less defined than for paired-pulse measures (
11,
15,
16).
These single-pulse TMS and paired-pulse TMS measures appear useful in detecting abnormalities in the inhibition:excitation ratio in patients with epilepsy. Data from published reports where parameters derived from TMS-EMG in patients with epilepsy were compared to values obtained from nonepileptic controls are summarized in
Table 53.2. Although findings vary between studies, and likely reflect subject and methodology differences, they do suggest that either primary or compensatory abnormalities in cortical inhibition:excitation ratio can be measured by TMS. In particular, pathologic suppression of intracortical inhibition (
Table 53.2) as detected by paired-pulse stimulation appears to be a common finding in patients with epilepsy.
In support of potential TMS-EEG application in measuring cortical excitability in patients with epilepsy, a recent experiment demonstrates that inhibition of the evoked EEG response over extramotor frontal and parietal cortex, analogous to LICI, can be recorded with a paired-pulse TMS-EEG paradigm (
37,
38). An interesting extension of these data may be to test whether extramotor LICI TMS-EEG abnormalities are present in the epilepsy population. However, as number of TMS-EMG experiments show motor cortex abnormalities in patients with extramotor and generalized epilepsies, further studies will be required to test whether interrogating focal cortical excitability outside of the motor cortex by TMS-EEG is of any greater clinical value than checking TMS-EMG measures (
39,
40 and
41).