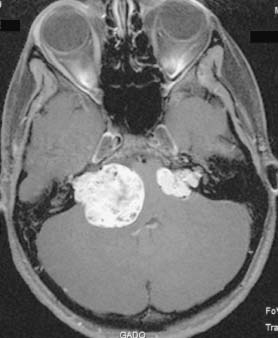
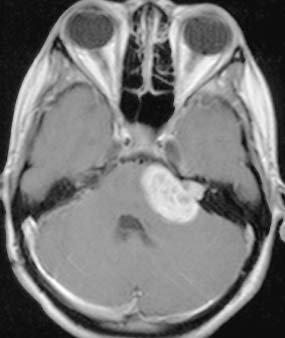
Section I Intracranial Pathology Fig. 1.1 T1-weighted postcontrast axial magnetic resonance image showing bilateral vestibular schwannomas. Note the severe compression of the brainstem. Fig. 1.2 T1-weighted postcontrast axial magnetic resonance image 2 years after surgery showing complete resection of the tumor on the right. At this point, the left-sided tumor was treated with gamma knife radiosurgery.
Case 1 Vestibular Schwannoma in Neurofibromatosis Type 2
 Clinical Presentation
Clinical Presentation
 Questions
Questions
 Answers
Answers
< div class='tao-gold-member'>
1 Vestibular Schwannoma in Neurofibromatosis Type 2
Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


