Vestibular schwannomas (e.g., acoustic neuroma, acoustic neurofibroma) are slow-growing, benign extra-axial tumors that arise commonly from the superior vestibular portion of the eighth cranial nerve (CN VIII). Vestibular schwannomas comprise 8% to 10% of intracranial tumors. Tumors may arise either sporadically (95%) or in association with neurofibromatosis type 2 (NF2). The incidence of sporadic cases is believed to be 1 per 100,000 personyears, with a median age of 50 years. As a result of the prevalence of magnetic resonance imaging (MRI), the incidence of vestibular schwannomas has increased recently, whereas the typical size at diagnosis has decreased.
PATHOBIOLOGY
Vestibular schwannomas are histopathologically benign tumors that grow slowly from the Schwann cell sheath surrounding the vestibular branch of CN VIII. Tumors are composed of Antoni A (narrow elongated bipolar cells) and Antoni B fibers (loose reticulated pattern of cells). Verocay bodies are frequently seen and consist of acellular eosinophilic areas surrounded by parallel arrangements of spindle-shaped Schwann cells.
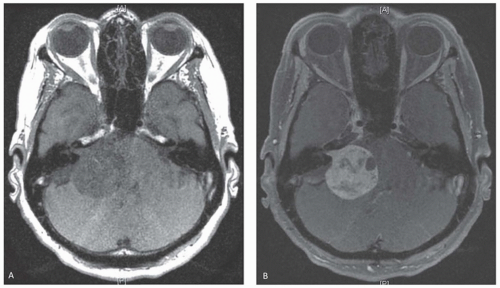
FIGURE 102.1 Vestibular Schwannoma. A: T1-weighted axial MRI before contrast shows large hypo intense mass within the CPA angle exerting mass effect on the brainstem. B: T1-weighted axial MRI post-contrast shows a vestibular schwannoma with expansion of the internal auditory meatus.
Vestibular schwannomas are typically unilateral lesions. Bilateral vestibular schwannomas occur in less than 5% of patients and are a defining characteristic of NF2, an autosomal dominant disorder involving the NF2 gene located on chromosome 22 band q11-13.1. This gene normally encodes the protein merlin (schwannomin), which is thought to play a role in membrane stability through interactions with cytoskeletal and integral membrane proteins. Loss of function of merlin in Schwann cells has been associated with both sporadic and NF2-related vestibular schwannomas, and the gene is often considered a classic tumor suppressor. Cytologically, vestibular schwannomas that arise in NF2 are identical to sporadic cases but with a greater tendency to infiltrate the nerve rather than displace it. In addition to patients with bilateral lesions, any patient younger than 40 years of age with a unilateral vestibular schwannoma should also undergo evaluation for NF2.
Tumors often originate within the internal acoustic meatus (intracanalicular; Fig. 102.1) and may extend into the cerebellopontine angle (extracanalicular). Mass effect from extracanalicular tumor may compromise function of cranial nerves, brain stem nuclei, and the cerebellum. Tumors typically follow three growth patterns: (1) no or very slow growth; (2) slow growth (2 mm/yr linear growth on imaging studies); or (3) fast growth (> 8 mm/yr) as a result of the enlargement of cystic components or rarely, intratumoral hemorrhage.
TABLE 102.1 Symptoms in Vestibular Schwannoma (1,000 Patients)
Symptoms
%
Hearing loss
95
Tinnitus
63
Dysequilibrium/vertigo
61
Headache
12
Trigeminal nerve disturbance
9
Facial paresis
5.2
Caudal cranial nerve disturbances
2.7
Change of taste
2
Diplopia
1.8
From Matthies C, Samii M. Management of 1000 vestibular schwannomas (acoustic neuromas): clinical presentation. Neurosurgery. 1997;40(1):1-9; discussion 9-10.
CLINICAL FEATURES
Vestibular schwannomas most commonly present with progressive unilateral hearing loss, characterized by difficulty with speech discrimination, especially when talking on the telephone. The next most common symptoms include tinnitus, followed by balance difficulties (Table 102.1). This triad of symptoms is related to pressure on the eighth nerve complex in the internal auditory canal. Other presenting symptoms include facial paralysis, trigeminal neuralgia, and rarely, hydrocephalus and brain stem compression in the setting of larger tumors. Although this constellation of symptoms may occur with any mass in the cerebellopontine angle, including meningioma, cholesteatoma, or trigeminal neuroma, only rarely will these other lesions cause tinnitus or hearing dysfunction.
DIAGNOSIS
Patients with hearing loss often undergo audiometric evaluation with pure tone audiogram and speech discrimination evaluation. Those with vestibular disturbances may undergo vestibular testing. Hearing loss is typically insidious and progressive, with 70% of patients demonstrating a high-frequency loss pattern and impaired word discrimination (especially noticeable in telephone conversation). Tinnitus is usually high-pitched. Weber test lateralizes to the uninvolved side, and Rinne test will be positive on both sides if there is enough preserved hearing.
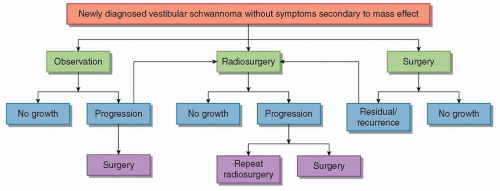
FIGURE 102.2 Treatment algorithm for vestibular schwannoma management.
Asymmetric sensorineural hearing loss, or defects in other cranial nerves, indicates the need for imaging. Gadolinium-enhanced MRI is the gold standard for diagnosing vestibular schwannomas. Tumors enhance brightly, and an origin within the internal auditory canal suggests vestibular schwannoma rather than meningioma. Contrast-enhanced computed tomography (CT) can also be used to diagnose vestibular schwannomas greater than 15 mm in diameter for patients who cannot undergo MRI.
TREATMENT
The goal of treatment is to cure the tumor while preserving intact neurologic function. Following diagnosis, patients with vestibular schwannomas have several options for managing their tumor including observation with serial imaging, stereotactic radiosurgery (SRS), fractionated radiotherapy (RT), and microsurgery. Selection of treatment modality depends on tumor size, symptoms, patient age, patient health, and patient preference. Figure 102.2 represents a decision tree following initial diagnosis of vestibular schwannoma. In general, noncystic, non-NF2 intracanalicular tumors or cerebellopontine angle (CPA) tumors 20 mm or smaller may be followed with serial imaging and hearing tests. Tumors larger than 15 to 20 mm should be treated. NF2 patients present a challenge and should be evaluated on a case-by-case basis.
Observation/Expectant Management
Observation with serial clinical assessment and follow-up MRI to monitor for signs of tumor growth is an option in the management of vestibular schwannoma. Patients using this approach are monitored using MRI until progression of symptoms or tumor growth warrants more invasive treatment. Imaging is performed every 6 months for 2 years after diagnosis. If stable, imaging occurs annually until year 5 after diagnosis and then occurs at year 7, 9, and 14 after diagnosis. However, observation is not without risk, as tumor growth rates and progression of symptoms are not predictable. By 10 years, most clinical experience demonstrates that the majority of patients will have tumor growth and progression of symptoms. Therefore, the “wait and scan” approach should mainly be used in older patients and those whose medical comorbidities preclude other treatment options.
Stereotactic Radiosurgery
Radiosurgery is a therapeutic option that improves tumor control and hearing preservation compared with observation in patients presenting with small tumors (< 30-mm diameter), serviceable hearing, or in those who wish to avoid surgery due to preference or anxiety. A dose of 12 to 13 Gy is prescribed typically and associated with improved hearing preservation. Long-term tumor control rates ranging from 91% to 98% have been reported in large series after radiosurgery, with 1.6% to 4.2% ultimately requiring resection for progressive enlargement. When applied early after diagnosis, long-term hearing preservation is achieved in greater than 60% of patients with doses of 13 Gy or lower, with higher rates achievable with intracanalicular tumors. Minimizing the radiation exposure to nearby structures (i.e., the cochlea, semicircular canals, and brain stem in larger tumors) minimizes morbidity rates associated with radiosurgery without sacrificing efficacy. Preservation of facial and trigeminal nerve function is also possible in the majority of patients.
For smaller tumors, hearing preservation and tumor control rates are equivalent following radiosurgery or surgical resection. However, radiosurgery is more effective than surgical resection in preserving postoperative facial function and is associated with lower rates of trigeminal neuropathy and other treatment-associated morbidity. In addition, hospital lengths of stay and management costs are less after radiosurgery and in general, hospital postoperative functional outcomes and patient satisfaction have been found to be greater after radiosurgery when compared with microsurgery.
Surgical Resection
Microsurgical resection remains the best cytoreductive therapy for vestibular schwannomas and is generally indicated in the setting of tumor progression after previous interventions and for those with large tumors (> 30 mm diameter). In particular, microsurgery remains the preferred treatment for large lesions causing mass effect and obstructive hydrocephalus. Additional treatment is necessary in less than 2% of cases after microsurgical treatment. Facial nerve function may be preserved in more than 95% of patients with small tumors less than 20 mm, with rates of preservation dropping in the setting of tumors larger than 30 mm. Serviceable hearing, otherwise known as useful hearing, is assessed using the combined results of pure tone audiogram that evaluates the functionality of hearing and speech discrimination tests. Serviceable hearing is maintained in 32% to 44% of cases, with rates closer to 50% in the setting of tumors less than 30 mm. Recent data suggest that planned neartotal or extensive subtotal resections, followed by radiosurgery for residual tumor, may be appropriate for large tumors, with excellent rates of facial nerve preservation and functional outcomes and no decrease in tumor control.
TABLE 102.2 Clinical Syndromes Associated with Metastases to the Skull Base