Chapter 32D Clinical Neurophysiology
Neuromodulation
Neuroscientists have defined neuromodulation as a dynamic process wherein a substance, usually a neurotransmitter, affects neuronal function by its action on the synapses and by modulating the response of the cell to other inputs, with potentially important behavioral implications. Neuromodulation has come to be more broadly defined as a process whereby the central, peripheral, or autonomic nervous system is electrically excited, inhibited, stimulated, modified, regulated, or therapeutically altered to achieve the desired effect (Krames et al., 2009). An ongoing dynamic process that affects targeted neural networks and utilizes electrical or neuropharmacological stimulation, neuromodulation may offer clinical outcomes that are potentially modifiable by simply adjusting stimulation parameters (Holsheimer, 2003). Other relevant terms that have been used to describe neuromodulation and its related techniques have included neurostimulation, neuroaugmentation, neuroprosthetics, functional electrical stimulation (FES), assisted technologies, and neural engineering. The International Neuromodulation Society has further defined neuromodulation “as a field of science, medicine and bio-engineering that encompasses both implantable and non-implantable technologies that may be electrical or chemical, and serve the purpose of improving quality of life and the overall functioning of humankind” (Sakas et al., 2007a).
Multiple specialties use neuromodulatory techniques for a variety of clinically relevant issues including augmentation of vision and hearing, cardiac pacing, and treating movement disorders, pain, epilepsy, stroke, depression, addiction, and gastrointestinal (GI) and urinary conditions. For more information on the history and classifications of neuromodulation, please go to www.expertconsult.com.
History of Neuromodulation
The first medical use of electricity was described by Scribbonius Largus, a Roman who used the electric torpedo fish to treat headache and address gout (Stillings, 1973). Modulation of brain activity by electrical stimulation of the dog motor cortex in an effort to induce limb movements was reported in 1870. Subsequently, stimulation of the human brain was tested by Sir Victor Horsely, who applied his technique to the occipital lobes (Vilensky and Gilman, 2002). Later, electrical stimulation was introduced as a more routine procedure. Brain lesions and biopsies were guided by what was referred to as “test stimulation,” and this technique was later refined by Spiegel and Wycis when they introduced the stereotactic head frame (Spiegel et al., 1947), which added precision to the targeting of very small brain regions. Movement disorder neurostimulation and psychosurgery continued to be performed in the 1960s and 70s; these surgeries used test or macrostimulation and then followed with alcohol-induced lesions and/or radiofrequency lesions once the target was carefully identified (Feldman and Goodrich, 2001; Guridi and Andres, 1997).
The potential benefits of chronic stimulation of brain targets have been refined by laboratory studies as well as intraoperative human stimulation. Following Melzack and Wall’s “gate theory” for pain (Melzack and Wall, 1965), implantable spinal cord neurostimulation and later brain stimulation were introduced as rational ways to “neuromodulate” relevant circuitry. Similarly in 1987, Professor Alim Benabid ameliorated a tremor in a chronic pain patient. Benabid left a chronic stimulating lead in place, and this has been considered the birth of a new application for neuromodulatory technology (Benabid et al., 1987). The current field of neuromodulation has evolved to include deep brain stimulators, pacemakers for breathing, urinary control systems, sacral nerve stimulation, cortical control systems, cochlear implants, visual prostheses, and neurorehabilitaton devices. All of these neuromodulatory devices have evolved in a relatively short period of time, and many have enhanced quality of life for various patient populations.
Classification
Although few attempts have been made, rapid proliferation and evolution of this field created a need for a more formal classification scheme for neuromodulation and related technologies. Classification has not been officially standardized, but many publications have recommended the following strategies: classified broadly (electrical versus pharmacological), classified by purpose (therapeutic, rehabilitative, or assistive), classified by body region placed (external, noninvasive versus internal, implanted), classified by directionality/functionality (open loop versus closed loop), and classified by nervous system (central versus peripheral) (Hatzis et al., 2007).
Neuromodulatory devices are thought to primarily work by modifying nervous signals in an effort to produce some sort of biological response (Sakas et al., 2007a). Some devices have been developed for neuropharmacological purposes and may thus be used to apply drugs in small doses to maximize benefits and limit side effects. Other devices may act in parallel with damaged parts of the nervous system to facilitate functional restoration. Facilitation can be provided by prosthetics and by neuro-orthotics specifically designed to take over a particular nervous function (Stieglitz, 2007).
It is important to distinguish between therapeutic devices and rehabilitative devices. Therapeutic neuromodulatory devices are generally used to maintain vital bodily functions. Rehabilitative devices, on the other hand, usually focus on assisting an individual to regain a bodily function. Therapeutic devices may be lifelong, whereas rehabilitatives may or may not be long-term adjuncts. Traditionally, many devices have used open-loop stimulation (constant neurostimulation without any feedback); however, smarter closed-loop devices (still in their infancy) may eventually have the potential to maximize battery life and minimize side effects (Halpern et al., 2008).
Applications of Neuromodulatory Devices
The human nervous system is composed of many complex and distinct neural networks. These networks may include chemical and electrical synapses, and they may communicate both within and between network structures. The structure and subsequently the behavior of these neural networks may be “shaped by the extrinsic as well as intrinsic neuromodulatory effects that include those of hormones and neurotransmitters” (Destexhe et al., 2004; Katz and Frost, 1996). The classifications and applications of neuromodulation devices are summarized in Table 32D.1.
Table 32D.1 Classification of Neuromodulation Devices
| Stimulation | Electrical (e.g., DBS, MCS, SCS, PNS, TENS) |
| Pharmacological (e.g., infusion pumps) | |
| Application | Neuroprosthesis (auditory, retinal implants, phrenic/sacral nerve stimulators) |
| Neuro-orthosis | |
| Purpose | Therapeutic (neurostimulators for breathing, bladder and bowel functions) |
| Rehabilitation (neurostimulators for extremity functions) | |
| Placement | Implanted and invasive (DBS) |
| External and noninvasive (neurostimulators for extremity functions) | |
| Control and directionality | Open-loop (VNS, DBS) |
| Closed-loop (NeuroPace) | |
| Effect on nervous system | Central nervous system (DBS) |
| Peripheral nervous system (PNS) |
DBS, Deep brain stimulation; MCS, motor cortex stimulation; PNS, peripheral nerve stimulation; SCS, spinal cord stimulation; TENS, transcutaneous electrical nerve stimulation; VNS, vagus nerve stimulation.
Neurostimulation devices may involve either the application of deep brain/spinal cord leads or surface leads, or alternatively they may use direct stimulation of the spinal cord and/or peripheral nerves. Precisely placed leads may be connected via an extension cable to a pulse generator and ultimately to some sort of power source (battery). This process has the potential to generate the necessary electrical stimulation and to (hopefully) provide clinically relevant benefits (Panescu, 2008). Signals can be excitatory, inhibitory, or both (e.g., excite fibers and inhibit cells) (Vitek, 2002).
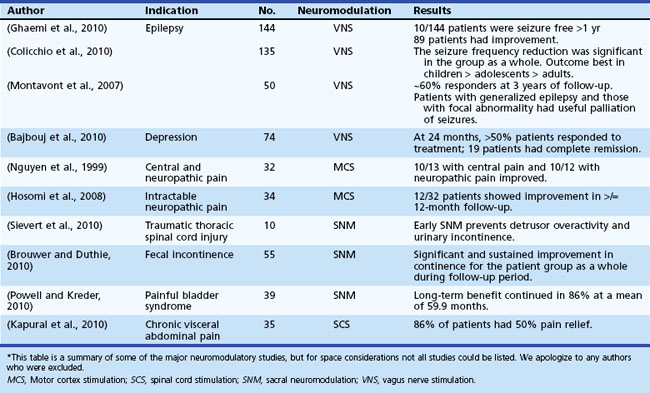
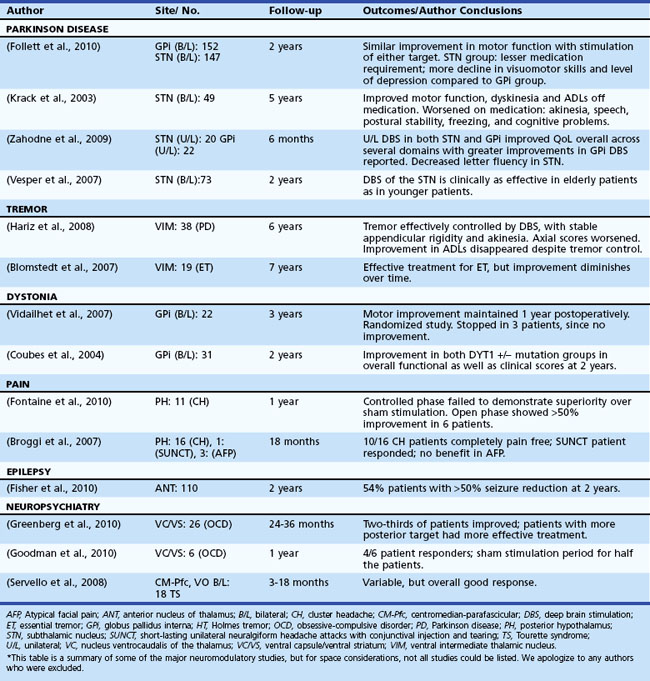
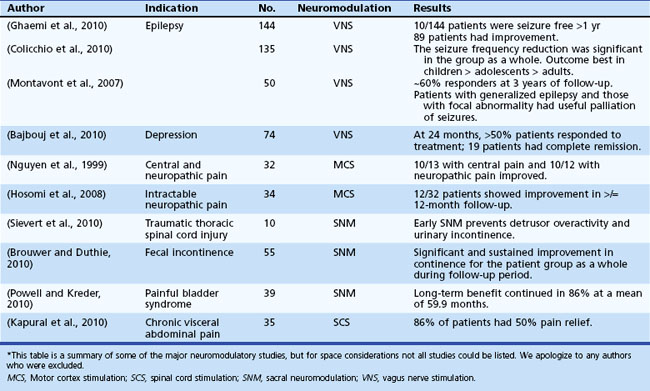
Table 32D.2 offers a selected summary of the literature on deep brain stimulation (DBS) neuromodulation for movement and neuropsychiatric disorders, and Table 32D.3 is a selected summary of the literature on non-DBS neuromodulation.
Extended versions of these tables are available online at www.ExpertConsult.com.
Table 32D.2 DBS Neuromodulation: Selected Summary of the Literature* (See Extended Online-Only Version)
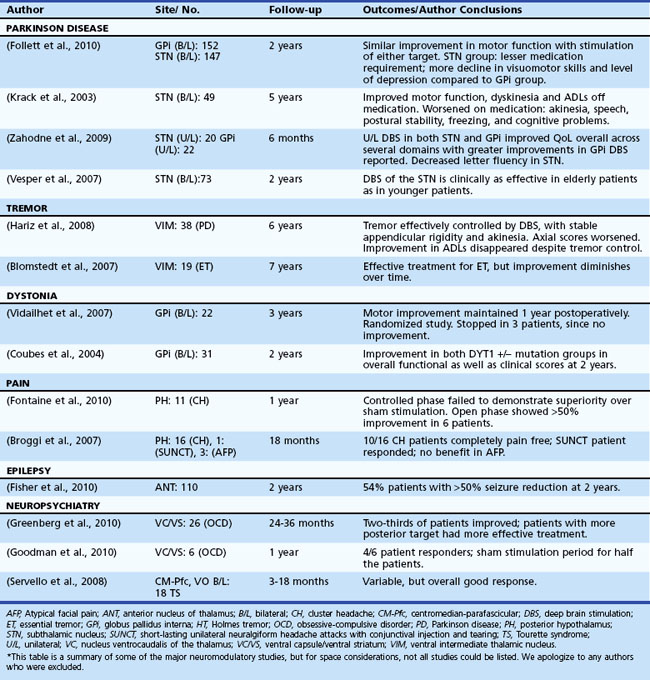
Table 32D.3 Non-DBS Neuromodulation: Selected Summary of the Literature* (See Extended Online-Only Version)
Motor Cortex Stimulation
Motor cortex stimulation (MCS) was utilized by Tsubokawa and colleagues, who originally presented this option as a possible safer alternative to DBS surgery in Dejerine syndrome (central thalamic pain syndrome) (Tsubokawa et al., 1991). It has been hypothesized that MCS induces antidromic activation of the sensory cortex, and this results in inhibition of the abnormal burst activity in a damaged and possibly deafferented sensory thalamus. Imaging studies “on” and “off” MCS have shown interesting blood flow changes within the ventrolateral (VL) tier of the thalamus, the medial thalamic regions, and the anterior cingulated cortex, orbitofrontal cortex, anterior insular cortex, and upper brainstem. Perhaps the most interesting aspect of post-MCS imaging has been the finding that blood flow does not seem to increase in the somatosensory cortex. Interpretations of this data have been variable, but the latest suggestions are that descending projections from the cortex to the thalamus can be activated and potentially lead to changes in basal ganglia pathophysiology within a loop responsible for both pain and emotional aspects of pain (Garcia-Larrea et al., 1999). It is thought that MCS may primarily stimulate γ-aminobutyric acid (GABA)-ergic interneurons that are found to be in parallel orientation to other layers of the cerebral cortex (Manola et al., 2007). Researchers have noticed that pain relief (≥40%\xE2\x80’50% improvement on the visual analog scale) from MCS seems to be greatest in cases where the corticospinal tract is found to be relatively intact (Katayama et al., 1998). Interestingly, when MCS is applied, patients with paretic extremities and concomitant central pain problems may have noticeable benefits in motoric weakness, rigidity, and spasticity. These improvements can, in select cases, aid in improving rehabilitation potential (Katayama et al., 1998).
MCS has been applied in cases of pharmacoresistant trigeminal neuralgia, painful peripheral neuropathy, and certain spinal cord pathologies. A greater than 50% pain relief has been reported in various studies of patients with central and neuropathic pain (Katayama et al., 1998; Nguyen et al., 1999). Data from randomized controlled studies for any application of MCS are lacking, however. There appears to be a large placebo effect with the therapy, and it has been noted that the effects may wane over time (Fontaine et al., 2009; Lima et al., 2008). Motor cortex stimulation has been attempted for therapeutic treatment of Parkinson disease (PD) and multiple system atrophy (MSA), but to date, results have been disappointing (Gutierrez et al., 2009; Kleiner-Fisman et al., 2003).
Transcranial Magnetic Stimulation
Information on transcranial magnetic stimulation (TMS) can be found in Chapter 32C as well as in the online version of this chapter at www.ExpertConsult.com.
Transcranial magnetic stimulation (TMS) is a noninvasive device consisting of an electromagnetic coil which when placed on the scalp, converts brief, high-current electrical activity into a rapidly cycling magnetic field. The magnetic field courses unimpeded through the scalp to induce localized intracranial electric current and thereby depolarizes the neurons, resulting in excitation or inhibition of the underlying neuronal circuit (Beric, 1993). Specific stimulation parameters such as current amplitude, duration, and direction can be used to calculate delivery of energy to a particular area in the brain. Repetitive TMS (rTMS) up to 60 Hz can be used to produce incrementally greater clinical effects (Andrews, 2003). The effects in general seem to be excitatory at fast frequencies (>1 Hz) and inhibitory at slow frequencies (≤1 Hz), and this may be similar to the published effects of long-term potentiation and long-term depression (Chen et al., 1997; Pascual-Leone et al., 1994). The state of brain activity, the integrity of the neural networks, and the interactions of the TMS with the targeted brain tissue can all be important in producing positive effects. Specific TMS stimulation parameters may also have positive and negative effects. The biological mechanism of action of TMS is not well understood, although changes at genetic levels and changes in concentrations of various neurotransmitters including monoamines, GABA, and glutamate have been suggested and may lead to corticospinal excitability and/or intracortical inhibition (Albert et al., 2009).
TMS has found applications in mapping the motor cortex and in treating post-stroke patients and several neurological disorders (movement disorders, neuropsychiatric disorders, epilepsy, tinnitus, and migraine), with varying degrees of success and failure. Some TMS targets include various regions of motor cortex in Parkinson disease (PD), dorsolateral prefrontal cortex (DLPFC) in depression, and left temporoparietal cortex in schizophrenia (Rossini and Rossi, 2007).
Different stimulation strategies for treatment of drug-resistant major depression have been attempted by randomized trials, suggesting the possibility of short-lived, clinically significant antidepressant effects (stimulation of the left DLPFC). Favorable responses to TMS may be predicted by previous medication treatment failures, lack of comorbid anxiety, and shorter duration of the current depressive episode (Avery et al., 2007; George, Lisanby et al., 2010; Lisanby et al., 2009; O’Reardon et al., 2007), although more data are needed to better understand positive clinical responses to TMS. It is unclear, however, whether the benefits of such treatment strategies will be sustained or whether longer-duration treatments may result in higher response and remission rates (Lam et al., 2008). A recent meta-analysis of rTMS for various neuropsychiatric disorders has supported its role in treating depressive symptoms and auditory hallucinations and addressing the negative symptoms of schizophrenia (Slotema et al., 2010). High-frequency rTMS has been shown to improve short-term motor scores in PD, potentially by enhancing motor cortex excitability (Elahi et al., 2009; Hemond and Fregni, 2007). In post-stroke patients, stimulation of the lesioned hemisphere (or alternatively, inhibition of the contralateral hemisphere) may aid in rehabilitation efforts. Repetitive TMS is also thought to have a potential role in treating neuropathic or visceral pain (Hemond and Fregni, 2007).
Seizure is the major adverse effect raising treating clinicians’ concern when applying TMS. Careful selection of patients may help avoid this complication. In general, patients with increased intracranial pressure, a metallic object(s) embedded in their head, or heart disease should avoid TMS. Other notable and not uncommon side effects from the stimulation include headaches, tinnitus, and facial muscle twitches (Andrews, 2003).
Deep Brain Stimulation
Over the last 2 decades, chronic DBS has become routine for several diagnoses in neurological practice (e.g., PD, dystonia, essential tremor) and has been used experimentally for selected neuropsychiatric indications (e.g., obsessive compulsive disorder [OCD], depression, Tourette syndrome [TS]). Interestingly, as early as the 1950s, temporary DBS electrodes were implanted into the septal region for pain control, and they were reported to have beneficial effects (Hamani et al., 2006). Over the ensuing years, there were various attempts at DBS, with most documented experiences revealing its usefulness in test stimulation prior to ablating brain lesions (Blomstedt and Hariz, 2010). In 1987 when Professor Benabid was operating on a chronic pain patient, he noticed that the patient’s tremor improved during test stimulation, and he decided to chronically stimulate this patient. Over the ensuing 2 decades, multiple DBS placements into multiple brain regions for a variety of clinical indications have occurred (Awan et al., 2009).
High-frequency stimulation (HFS) has been thought to effect a basal ganglia network–wide change, acting as a sort of informational lesion (Birdno and Grill, 2008; McIntyre et al., 2004a; McIntyre et al., 2004b). Thus, PD computer model systems have been developed to attempt to elucidate the mechanism of action of DBS (Birdno and Grill, 2008; McIntyre et al., 2004a; McIntyre et al., 2004b). HFS has been hypothesized to result in a decoupling of the cellular and axonal output within a thalamocortical relay circuit. The firing rates and patterns of the cell body may be suppressed, while the fibers and fibers of passage may be excited. DBS may ultimately effect a corticostriatopallido-thalamocortical (CSPTC) network and result in upstream as well as downstream changes within this complex basal ganglia network (McIntyre and Hahn, 2010). The specific effects of an electrical field are thought to reflect changes relative to the position and orientation of the axon to the actual DBS lead. Also, the electrical field is thought to exert trans-synaptic influences (McIntyre et al., 2004a; McIntyre et al., 2004b). The clinical benefits of DBS have been hypothesized to be due to more than just local neurotransmitter release (Stefani et al., 2005); however, several authors have argued that there is a collective effect and that transmitter release may be very important to the mechanism of action (Dostrovsky and Lozano, 2002; Lee KH et al., 2004; Vitek, 2002). Animal models of DBS have revealed increased extracellular concentrations of glutamate and GABA (Windels et al., 2003) and, most recently, adenosine and dopamine (Chang et al., 2009; Shon et al., 2010). Depolarization blockade, synaptic inhibition, and synaptic depression (McIntyre et al., 2004a; McIntyre et al., 2004b) have also been proposed to play a role in the potential mechanisms of action of DBS.
Selective placement of the DBS leads within different anatomical regions and different somatotopies may affect the neuronal network and, in the best possible cases, lead to improvement in clinical symptoms. For example, the placement of DBS electrodes in the ventralis intermedius nucleus of the thalamus for essential tremor may have an effect on an abnormal thalamocortical oscillatory loop and ultimately suppress tremor (Birdno et al., 2007). Similarly in PD, placement of a DBS lead in the ventralis intermedius may improve tremor; however, to affect bradykinesia and rigidity, one must either implant the ventralis oralis thalamic nucleus or, alternatively, either the subthalamic nucleus or globus pallidus internus (Mann et al., 2009; Oh et al., 2002).
DBS is a relatively simple technology. In its current form, it involves placement of a quadripolar (four contacts) lead into a specific and predetermined brain target. The lead is usually connected to a neurostimulator placed subcutaneously under the clavicle, although the battery can be placed in a multitude of regions. The neurostimulator can then be programmed or adjusted to tailor a setting to an individual patient. There are thousands of different combinations that may be chosen, and the voltage, frequency, and pulse width may be liberally changed. The optimal settings are patient and symptom specific, and they usually require that patients be reprogrammed frequently for the first 4 to 6 months and medications as well as stimulation monitored (Ondo et al., 2005; Rodriguez et al., 2007).
Each disorder or symptom considered for treatment with DBS should be carefully evaluated. Only a small fraction of any neurological or neuropsychiatric disorder may be eligible for this type of therapy. Most patients receiving DBS should be medication resistant, and they should undergo a complete multi-/interdisciplinary screening with a neurologist, psychiatrist, neuropsychologist, and neurosurgeon. Following screening, there should be a detailed interdisciplinary discussion about the goals of therapy (symptoms targeted, symptoms that will likely respond, symptoms not likely to respond). In cases of PD, patients should undergo an “off/on” levodopa medication challenge to determine which symptoms respond best to medication—these usually are the ones that respond best to stimulation (with the exceptions of tremor and dyskinesia). Risks and benefits of a potential DBS surgery, as well as the potential brain target(s), and unilateral versus bilateral DBS should all be carefully addressed in preoperative conversations with patients and families (Alberts et al., 2008; Kluger et al., 2009; Okun et al., 2004; Okun et al., 2007; Okun et al., 2009; Okun and Foote, 2004; Okun and Foote, 2009; Rodriguez et al., 2007; Skidmore et al., 2006; Ward et al., 2010). There are many potential adverse events that may occur as a result of DBS, some of which may constitute emergencies (Morishita et al., 2010).
Depending on the region of the world and the preference of individual surgical teams, leads and batteries may be placed in a single setting or may be staged (separate operating room procedures). One lead, two leads, or in exceptional circumstances, more than two leads may be implanted in a single session. One recent review of DBS hardware-related complications cited lead migration, lead fracture, lead erosion/infection, and lead malfunction as common occurrences (Lyons et al., 2004; Oh et al., 2002). DBS surgically related and stimulation-related complications can occur and may include (but are not limited to) hemorrhage, infections, strokes, seizures, paresthesias, dysarthria, hypophonia, dystonia, mood worsening, suicide, and worsening of comorbidities. Difficulty with verbal fluency and anger seem to be common sequelae in PD patients (Blomstedt and Hariz, 2005; Blomstedt and Hariz, 2006; Hariz et al., 2008a; Okun et al., 2008a; Saint-Cyr and Albanese, 2006). DBS teams must differentiate between lesion effects, stimulation-induced effects, and transient versus permanent neurological dysfunction. More DBS and device-related studies are needed to prospectively document all adverse effects; this constitutes a critical weakness of many published series (Hariz et al., 2008b).
Parkinson Disease
Parkinson Disease is a complex disorder thought to be the result of extensive loss of neurons and their projections within motor and nonmotor basal ganglia circuitry (Alexander et al., 1986). A rationale for neuromodulatory therapy has been developed as a result of models of basal ganglia physiology. Perhaps the most famous model reveals loss of dopaminergic neurons in the substantia nigra pars compacta, with a resultant abnormal neuronal activity in both the direct and indirect basal ganglia circuitry. These changes are thought to result in the genesis of many of the motor symptoms of PD. Initial treatment of PD is usually with dopaminergic therapy, though over time, disease progression may lead to limitations in medical therapy including such symptoms as wearing off between doses, on/off fluctuations, and hyperkinetic dyskinesia. Subthalamic nucleus (STN) or globus pallidus interna (GPi) DBS have been used to neuromodulate basal ganglia pathways and restore important functions in selected patients (Pahwa et al., 2005; Weaver et al., 2009). Studies are underway to define the selection criteria and help tailor the procedure for individual patients. To date, STN and GPi DBS have shown similar motor outcomes, but STN DBS may allow for larger dopaminergic medication reductions, and GPi DBS may provide better dyskinesia suppression and a relatively safer risk/benefit profile (Anderson et al., 2005; Follett et al., 2010; Mikos et al., 2010; Okun and Foote, 2009; Zahodne et al., 2009). These conclusions, however, will need to be bolstered by randomized clinical studies.
Long-term efficacy of DBS in PD has been good overall, but in all cases, the disease progresses. An important guideline is that symptoms that respond to levodopa continue to respond to DBS, with the exceptions of tremor and dyskinesia, which may have persistent benefits (Krack et al., 2003; Schüpbach et al., 2005; Wider et al., 2008).
Dystonia
Dystonia results from co-contraction of agonist and antagonist muscles, and patients may experience involuntary repetitive movements that result in twisted and sometimes painful postures. Dystonia may be focal, segmental, or generalized based on the body region affected. Other classification systems use age of onset or etiology. The most studied dystonia syndrome has been DYT-1 genetic dystonia; when the DYT-1 gene is expressed prior to age 26, the disease manifests. In those who live asymptomatic past age 26, the mutation (which occurs in the torsin A gene and is due to deletion of the GAG code) remains clinically silent (a carrier state) (Bressman, 2003). This is a phenomenon referred to as incomplete penetrance.
Lesion surgery (pallidotomy and thalamotomy) have both been successfully employed for various primary and secondary dystonias (Lozano et al., 1995; Yoshor et al., 2001), though most centers prefer DBS because bilateral lesions may result in speech or cognitive issues (Hua et al., 2003; Ondo et al., 1998). DBS therapy is mainly performed in the pallidal (GPi) target, because stimulation in this region has provided a reasonable alternative to lesion therapy. Most DBS cases have responded best if the dystonia has been of primary origin, although selected secondary dystonias as well as tardive dystonia have had meaningful improvements in small series (Coubes et al., 1999; Kumar R et al., 1999; Kupsch et al., 2003; Tronnier and Fogel, 2000; Vercueil et al., 2001). There have been two large randomized trials to date that addressed primary generalized dystonia, and both short- and long-term outcomes have been promising (Coubes et al., 2004; Vidailhet et al., 2005; Vidailhet et al., 2007). Additionally, the number of indications has been expanding within dystonia (e.g., cerebral palsy), and the number of brain targets also continues to expand (e.g., STN).
One interesting and unique aspect of DBS for dystonia has been the phenomenon that in many cases, the effects seem to be delayed and appear gradually after stimulation initiation (weeks to months). It has been hypothesized that this phenomenon may be the result of neuroplasticity, but its true mechanism remains a mystery. The other evolving story in dystonia DBS has been the use of lower stimulation frequencies for selected cases (Alterman et al., 2007). Which cases may respond to lower frequencies remains an area of investigation.
Tremor
Tremor has been broadly defined as an involuntary and rhythmic oscillation of a body part and has been classified according to its etiology and/or characteristics (e.g., phenomenology, physiology, etc.). It has been hypothesized that physiological disturbances in the cerebellothalamic and pallidothalamic pathways may be the genesis of some but not all tremor subtypes. According to Deuschl et al. (2001), four pathophysiological mechanisms are proposed to result in tremor: mechanical oscillation of the extremity, reflex activation of the oscillation network, central oscillation, and a disturbance in the regulatory feed-forward or feedback loops of an oscillation network. The ventralis intermedius (VIM) nucleus of the thalamus, which takes its input from the cerebellum, forms a vital piece of this regulatory network and has been frequently targeted for high-frequency (≥100 Hz) DBS to address various medication refractory tremors, with the most common being essential tremor (Benabid et al., 1996). DBS therapy has been reported to have similar efficacy as thalamotomy (Schuurman et al., 2000), and it may have fewer short-term side effects but more long-term (device related) side effects when compared to lesion therapy. Although VIM DBS is preferred for pure essential tremor and certain cases of PD tremor, other cerebellothalamic and pallidothalamic pathways may be altered with DBS. For example, outflow (cerebellar/midbrain) tremor, posttraumatic tremor, and multiple sclerosis (MS) tremor have all been treated in small case series by either single or multiple leads in VIM, ventralis oralis posterior, or zona incerta (Foote and Okun, 2005; Foote et al., 2006; Papavassiliou et al., 2008). The exact target(s) for these more complex tremor disorders remain to be investigated.
Typically, unilateral VIM DBS has been employed to control medication-refractory tremor in a contralateral extremity. Unilateral DBS commonly results in side effects of ataxia and speech problems, and these issues may be more commonly encountered when bilateral DBS is used (Pahwa et al., 2006). Midline tremor, head tremor, and voice tremor seem to respond less consistently to DBS (Ondo et al., 2001). Longitudinal follow-up studies have revealed good long-term benefits, although there has been an emerging concern in the field about tolerance and disease progression (Blomstedt et al., 2007; Pahwa et al., 2006; Sydow et al., 2003; Zhang et al., 2010). Other indications such as cerebellar tremor, Holmes tremor, and MS tremor have had worse efficacy when compared to essential tremor, but these outcomes may change with the emergence of better targets, better technology, and multiple lead approaches.
Neuropsychiatric Disorders
Tourette Syndrome
Tourette syndrome (TS) is a complex neuropsychiatric disorder with a usual onset in childhood (mean age 7 years). The disorder is characterized most prominently by changing motor and vocal tics that must be present for at least 1 year and be marked by fluctuations in number, frequency, and complexity (Robertson, 2000). Patients frequently have associated behavioral abnormalities including anxiety, attention deficit hyperactivity disorder, self-injurious behavior, and obsessive-compulsive behavior, which may persist in their adult life even when motor and phonic tics decline or disappear (Jankovic, 2001; Leckman et al., 1998). Only a small minority of patients diagnosed with TS progress to disabling refractory tic disorder or to malignant TS that is unresponsive to medical and behavioral therapy (Cheung et al., 2007). Only a very select group of TS patients may be candidates for DBS.
Although the mechanisms that cause TS are unknown, abnormalities within the limbic and motor loops of the cortical-basal ganglia/thalamocortical circuitry that involve both dopaminergic and serotonergic neurotransmission likely contribute to the motor and behavioral manifestations in mild and severe TS cases (Albin and Mink, 2006; Wichmann et al., 2006). The centromedian-parafascicular (CM-PF) complex of the thalamus (Houeto et al., 2005), the GPi (both motor and non-motor territories), and the anterior limb of the internal capsule have all been targets for DBS therapy. To date, the GPi and the CM-PF seem to respond better than the anterior limb, but more careful studies, including characterization of individual targets, will be needed (Burdick et al., 2010; Flaherty et al., 2005; Maciunas et al., 2007; Porta et al., 2009; Servello et al., 2008; Shields et al., 2008; Visser-Vandewalle et al., 2003). The heterogeneity of patient populations and the small size of these studies have limited interpretation of reported successes and failures. Because of the special risks in this population, the Tourette Syndrome Association has published guidelines for selection of DBS candidates and for the preferred standardized outcome measures that should be employed if attempting these surgeries (Mink et al., 2006).
Depression
Severe refractory depression is much more common than any other potential patient group for DBS therapy. The loss of quality of life, the impact on lost work hours, and the suicide rate make neuromodulatory therapy an attractive alternative for a select group of these patients (Ward et al., 2010). DBS for medication-refractory depression remains investigational and should only be considered when medication, psychotherapy, and electroconvulsive therapy are not helpful, and when an institutional review board experimental protocol has been obtained. Experts have hypothesized that there is an abnormality in the corticostriatal-thalamic-cortical (CSTC) network in severely depressed humans, and that by lesioning or neuromodulating at specific nodes, clinical symptoms may be reduced (e.g., anterior cingulotomy, anterior capsulotomy, subcaudate tractotomy, limbic leucotomy). It has been reported that up to two-thirds of well-selected patients may benefit, but these data are highly preliminary and not inclusive of the entire population of depression patients (Greenberg et al., 2003). Neuromodulatory targets and outcomes have been rapidly emerging and may include subgenual cingulate gyrus/outflow tract, ventral capsule/ventral striatum, nucleus accumbens, and the inferior thalamic peduncle (Greenberg et al., 2010; Mayberg et al., 2005; Ward et al., 2010). To date, the most encouraging results have been achieved with area 25 (cingulate) and anterior limb internal capsule stimulation.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


