be relieved with a nasal corticosteroid spray, such as mometasone furoate, or systemic decongestants. Allergic rhinitis treatment involves identifying the allergens and desensitization, or antihistamine use during seasonal episodes, and topical steroids. If aggressive medical therapy fails, surgical approaches targeting nasal anatomic abnormalities predisposing recurrent infection may be considered.
TABLE 55.1 Etiologies of Facial Pain Including the Peripheral Nervous System and Tissues Innervated | ||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||

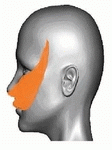

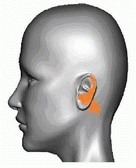
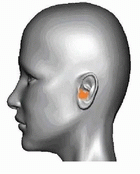
Pressure on tender trigger points, or nodular bands under the skin in muscles, tendons, or fascia, can cause pain locally or in other parts of the body via referral patterns. Initial muscle aggravation may be associated with oral habits or postural abnormalities.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


