The heterogeneous tumors collected in this chapter have been lumped together rather than split into more biologically meaningful groups, because that is how clinicians present them to the pathologist. The extra-axial “category” of tumors originates in radiology: current scans usually accurately distinguish tumors arising within brain or spinal cord parenchyma (intra-axial) from those arising outside it (extra-axial). Our job as pathologists is to further subcategorize these tumors by their biological behavior.
Extra-axial tumors grow in one of two places: either outside or inside the dura. Generally, extra-axial neoplasms growing inside the dura are benign or low-grade, whereas those growing outside the dura are malignant. These rules are not absolute: meningiomas can grow through and beyond the dura and metastatic prostate cancer has an affinity for the pachymeninges of the dura. Among the extra-axial intradural tumors, meningiomas and schwannomas make up the overwhelming number of cases; others represent just a small minority of tumors reaching the pathologist. These include the uncommon solitary fibrous tumor and the rarely resected neurofibroma. Outside the dura, metastatic carcinomas and direct extensions from primary carcinomas are most common; however, other tumors also occur in this region, including various sarcomas and chordomas. This chapter will primarily discuss meningiomas but will also discuss schwannomas. Smears of metastatic tumors and chordomas will be reviewed in subsequent chapters. The other, mostly rare tumors, are not further discussed in this book.
Meningiomas
Meningiomas have the dualistic distinction of being both boring and interesting. Some can be diagnosed in the wink of an eye. Others mimic many tumor types and require more extended study to identify and predict their behavior. These tumors have a well-known female predominance, in part due to their frequent expression of estrogen receptors. Many are asymptomatic; they can be found either fortuitously or at autopsy. Given the proliferation of brain scans for weak medical reasons and the high incidence of meningiomas in the normal population, many clinically silent tumors are now removed “because they are there” rather than because they are symptomatic. Most of these neoplasms grow very slowly. The brain has an amazing capacity to accommodate such slowly growing masses. As our brains age and atrophy, the slowly increasing space within our calvarium can accommodate ever-larger meningiomas. In the elderly, tumors arising in “noneloquent” areas occasionally become huge before clinically manifesting (Figure 10-1).
Radiologists usually accurately diagnose meningiomas; the tumors are dural-based, have a similar T1-signal intensity as brain, and enhance. These tumors arise along the entire neural axis, including within the spinal canal and posterior fossa. In the spinal canal, the tumors have a 10:1 female predominance. During development, the choroid plexus arises as an invagination of arachnoid, vessels, and ependyma; occasional meningiomas derive from these internalized arachnoid cells and arise within the ventricular space. The classic meningioma, proliferating from the dural-based arachnoid cells, shows a “dural tail” on neuroimaging (Figure 10-2). Like snow on a windowpane, a thickened dural tail forms a concave extension onto the bulging meningioma. Such tails sometimes are only visible in one of the three standard neuroimaging planes. Intact specimens display the same dural tails as the imaging. These tumors arise on the interior surface of the dura. Like normal arachnoid cap cells, the tumor cells infiltrate the dense connective tissue of the dura and firmly adhere to its surface. Intra-axial masses, such as a
metastasis to the cortex, form an acute or sharp angle with the overlying dura, rather than the more obtuse curve of a meningioma. Metastases invade into dura rather than arise from it.
metastasis to the cortex, form an acute or sharp angle with the overlying dura, rather than the more obtuse curve of a meningioma. Metastases invade into dura rather than arise from it.
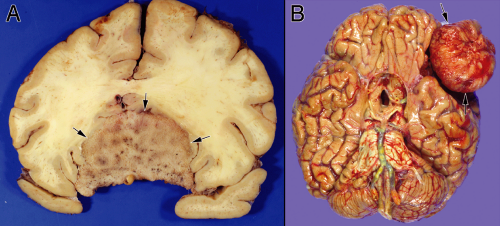 FIGURE 10-1. Massive meningiomas. A. This tumor was identified by neuroimaging in an 86-year-old cognitively normal woman. After a fall, she developed seizures, which lead to the imaging studies that found this tumor. The histologically benign meningioma encased her optic nerves, chiasm, and her cerebral arteries, without producing clinical effects on these structures. The patient also had a small, separate focus of metastatic carcinoma within her motor cortex. The metastasis produced her seizures; this meningioma was incidental. B. This woman had primary progressive aphasia. At autopsy, she had end-stage Alzheimer’s disease. This meningioma, lying over Broca’s area, was discovered at autopsy. Its relationship to her aphasia remains speculative. |
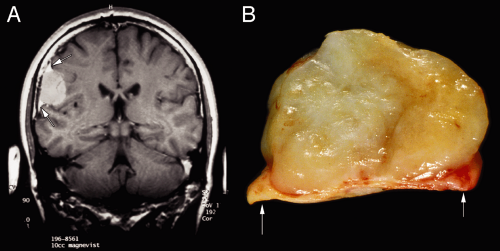 FIGURE 10-2. Comparison of meningioma radiology and gross specimen. A. The meningioma uniformly enhances and has distinct dural tails (white arrows). Notice how the brain shows almost no mass effect and only minimal edema around the tumor. B. An intact tumor has a similar dural tail (white arrows). The nodular growth of this meningioma is typical and reminiscent of a uterine fibroid. |
Many meningiomas have minimal impact on the brain. However, more aggressive or “atypical” meningiomas show increasing effects on their underlying brain parenchyma. The brain can adapt to a slowly growing tumor by gradually indenting, leaving the underlying tissue intact. In more rapidly growing tumors, the tissue fails to compensate. Aggressive tumors typically show mass effect, pushing brain from one region to another (Figure 10-3). In response to such injury, the underlying brain becomes edematous, which manifests as increased T2 or FLAIR signal. Finally, these tumors occasionally undergo internal necrosis, which produces a heterogeneous enhancement pattern on imaging. In many cases, the tumors will retain their dural tails.
Meningiomas grow in several different patterns. However, their building-block cells are strong, adhere to each other, and have interdigitating processes. Ultrastructurally, they contain abundant intermediate filaments, have desmosomes linking their membranes, and have wildly interleaved processes (Figure 10-4A). These features become important in understanding the cytology of their smears. On a larger scale, meningiomas commonly grow in several major patterns: as small whorls of cells (Figure 10-4B), in larger lobules akin to a syncytium (Figure 10-4C), or as fascicles of spindle cells (Figure 10-4D). Tumors can breed true, showing a single architecture, but more typically display several patterns. Cross-sections of these three-dimensional structures yields the common transitional (Figure 10-4E), meningothelial (Figure 10-4F), and fibroblastic patterns (Figure 10-4G).
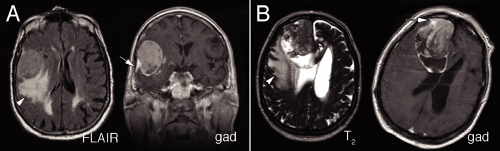 FIGURE 10-3. Radiology of atypical meningiomas. A. The patient had a meningioma that showed heterogeneous enhancement (gad) and produced significant edema in the surrounding brain parenchyma (FLAIR, white arrowhead). The tumor compressed the right brain and shifted it to the left. Notice how the tumor has retained its dural tail (white arrow). B. This massive tumor produced similar surrounding brain edema (T2, white arrowhead). Its enhancement pattern was complex (gad) and included some rim enhancement. This meningioma also compressed the underlying brain. The enhanced scan revealed a portion of the tumor’s small dural tail (white arrow). |
On macroscopic examination, meningiomas often have a lobular, whorled architecture, similar to uterine fibroids (Figures 10-2 and 10-5). During the crush stage of the smear, many meningiomas feel rubbery or tough. Preparing a good smear of such tumors requires increased pressure to break them apart. Others meningiomas are surprisingly soft and smear well. Even with adequate pressure, some tumors leave a thick clump at one end of the smear. If this is too bulky to coverslip, remove it with forceps and add it back to the original specimen.
To the unaided eye (put the slide up to the light), most meningiomas form clumps and cords of cells (Figure 10-6). Such clumps reflect the strong intercellular cohesion of these neoplasms. However, unlike other cohesive tumors (e.g., schwannomas), meningiomas invariably shed at least a few helpful cells or thinner clusters of cells (Figure 10-6, A and B, arrowheads). It is this chaff arising off the main clumps that is most fruitful for further examination. How these small groups interconnect and form whorls are the most distinguishing features of meningiomas. A low-power view also reveals the cohesiveness and penchant for these tumors to form thick bridges between clusters (Figure 10-6C, arrowheads).
Although generally thick areas of a smear yield little useful cytological information, they can give large-scale structural information about a tumor. In meningiomas, look for meningothelial lobules and the thick cellular bridges connecting them (Figure 10-7). These structural units remain firmly attached to their brethren, which produces globs of cells heaped on other globs of cells. The physical
shearing of these components leaves thick bridges of cells between them.
shearing of these components leaves thick bridges of cells between them.
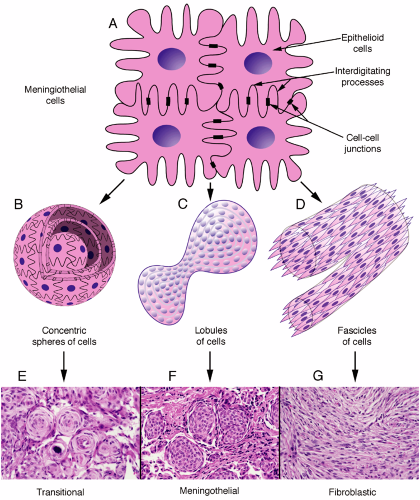 FIGURE 10-4. Major growth patterns of meningioma. A. Fundamental structural pattern in most meningiomas: abundant cytoplasm, densely interdigitating cell processes interconnected by desmosomes (dark boxes in membranes), and monotonous nuclei. These cells can grow as concentric spheres or whorls (B), in large lobules of cells (C), or as fascicles of spindle cells (D). Cells within whorls tend to degenerate and calcify, producing psammoma bodies. Within the large lobules, the interdigitating processes are below the resolution of a light microscope, which lends a syncytial appearance to the lobules. On histological sections, these major growth patterns lead to the major meningioma subtypes: transitional (E), meningothelial (F), and fibroblastic (G). |
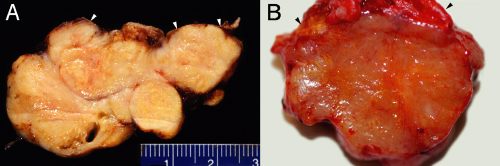 FIGURE 10-5. Macroscopic view of meningiomas. Both of these meningiomas are fleshy and lobulated. Large meningioma specimens often retain recognizable dura (white and black arrowheads), the tissue from which they arose. |
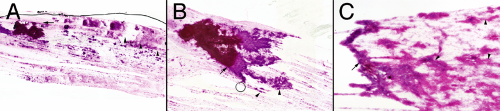 FIGURE 10-6. Meningioma smear field views from three different meningiomas. Each tumor left a large clump of cells at one end of the slide (black arrows). Unlike many cohesive tumors, meningiomas usually shed some diagnostic cells. These three tumors all shed smaller clumps of cells and some isolated cells (A and B, black arrowheads). C. Wide bridges of tissue span between the larger clumps of cells (black arrowheads). Notice how spicules of cells radiate out from the cellular clumps. (The line across the top of A and the circle in B are artifacts from the mounting medium.) |
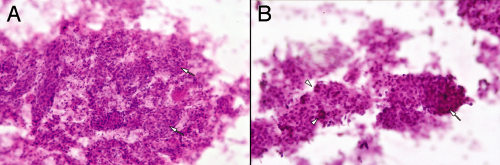 FIGURE 10-7. Thick zones in smears of meningiomas. Even the thick parts of a smear yield structural information about a tumor. Meningiomas often have meningothelial lobules or balls (A and B, white arrows) interconnected to each other. Like three-dimensional molecular models from chemistry class, these form balls heaped upon balls (B, arrowheads). |
At an intermediate magnification, meningiomas characteristically reveal their abundant cytoplasm, nuclear monotony, and connections between and among the cells (Figure 10-8). In the grade I tumors, nuclei are generally slightly oval and show minimal size variation. Occasional large or bizarre cells are often degenerative or “ancient” features, rather than anaplastic indicators. These intermediate microscopic powers are best to assess the variation in population of nuclei. The eye now resolves nuclear size and shape but also compares many nuclei in the same microscopic field. At the edges of the thicker regions, smearing rips tumor cells from the larger structures. Because the tumors typically have strong intercellular attachments, this ripping pulls the cytoplasm into broad sheets or processes (Figure 10-8




Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
