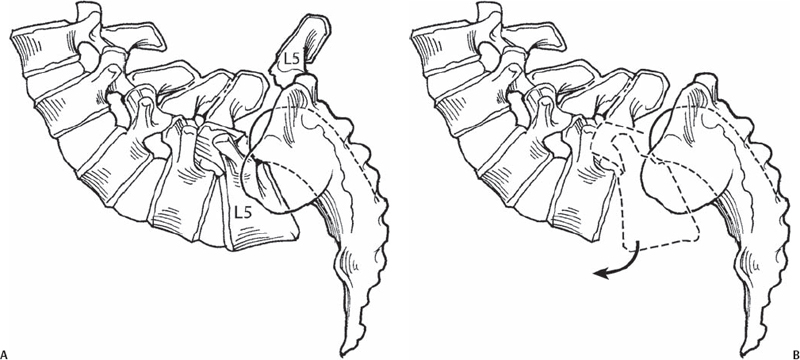
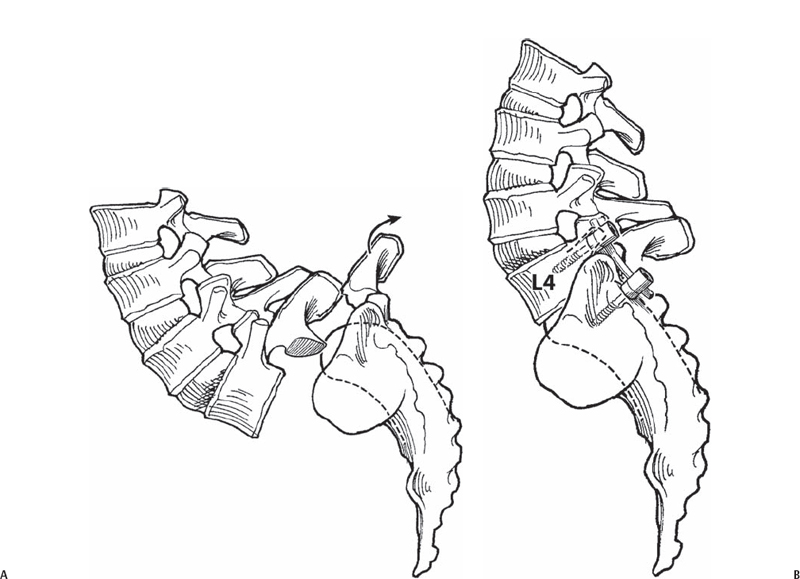
51 Vincent J. Devlin The Gaines procedure is a treatment option for spondyloptosis. This rare condition exists when the entire body of the L5 vertebra is located below the top of S1 on a standing lateral radiograph. The procedure requires a separate anterior and posterior approach to the lumbosacral junction. In the first stage, an anterior approach to the spine is performed, and the L5 vertebra, L5-S1 disk, and L4-L5 disk are removed (Fig. 51.1). In the second stage, the lamina and pedicles of L5 are removed to complete the L5 vertebrectomy, and the L4 vertebra is placed on top of the sacrum and held in place with pedicular fixation (Fig. 51.2). Fig. 51.1 (A) First-stage Gaines procedure. (B) The L5 vertebra, L5-S1 disk, and L4-L5 disk are removed. Fig. 51.2 Second-stage Gaines procedure. The lamina and pedicles of L5 (A) are removed to complete the L5 vertebrectomy, and the L4 vertebra (B) is placed on top of the sacrum and held in place with pedicular fixation. The treatment of spondyloptosis is a major challenge. The Gaines procedure is designed to restore sagittal plane alignment and minimize the risk of complications of cauda equina syndrome and L5 nerve root deficit. In addition, the morbidity associated with long-segment instrumentation and fusion is avoided. The procedure is indicated only for symptomatic spondyloptosis. Lesser degrees of vertebral slippage are not indications for this procedure. Contraindications to the procedure may be related to surgeon factors, facility support issues, and patient factors. The procedure should be performed by spine surgeons with extensive experience in all types of spondylolisthesis surgery. The operating room environment should provide appropriate support services including an experienced access surgeon, an adequate number of experienced surgical assistants, appropriate spinal instrumentation, and the capacity for intraoperative spinal monitoring. The patient’s symptoms and deformity should be sufficiently severe to warrant surgery, and the patient must be informed about the risks and complications of the procedure as well as realistic expectations and goals following surgery. Preoperative assessment includes detailed neurologic examination and appropriate imaging studies. Dynamic radiographs are utilized to assess reducibility of the deformity and to assess whether alternative procedures are a reasonable option. Neurodiagnostic imaging studies including magnetic resonance imaging (MRI) and computed tomography (CT) scans are important in planning surgical treatment. Patients with prior lumbar spine surgery, obesity, or prior abdominal surgery are more challenging surgical candidates. The first-stage procedure is performed with the patient in the supine position. The second-stage procedure may be performed on the same day or on a separate day based on multiple factors including duration of the first-stage procedure and intraoperative blood loss. If both procedures are performed on the same day, a Jackson table facilitates repositioning the patient to the prone position for the second-stage procedure. During the anterior procedure, the lumbosacral junction is located deep within the pelvis and is difficult to expose. Long-handled instruments (Cobb elevators, curettes, rongeurs, osteotomes) and a fixed abdominal retractor with long blades are essential for work in this area. During the posterior procedure, the posterior spine is located just beneath the skin, and careful and meticulous exposure is required to prevent iatrogenic neural injury.
Gaines Procedure for Spondyloptosis
Description
Key Principles
Expectations
Indications
Contraindications
Special Considerations
Special Instructions, Position, and Anesthesia
Tips, Pearls, and Lessons Learned
Key Procedural Steps
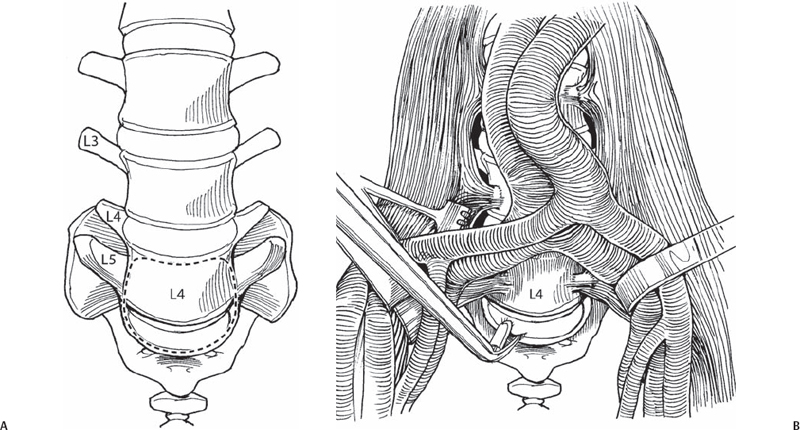
Anterior Approach (Fig. 51.3)
Related posts:
 Anterior Thoracic and Thoracolumbar Plating Techniques
Anterior Thoracic and Thoracolumbar Plating Techniques
 Anterior Cervical Corpectomy
Anterior Cervical Corpectomy
 Minimally Invasive Posterior Surgical Approaches to the Lumbar Spine Through Tubular Retractors
Minimally Invasive Posterior Surgical Approaches to the Lumbar Spine Through Tubular Retractors
 Anterior Lumbar Surgical Exposure Techniques
Anterior Lumbar Surgical Exposure Techniques
 Spondylolysis Repair (Pars Interarticularis Repair)
Spondylolysis Repair (Pars Interarticularis Repair)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


