Ataxia is characterized by incoordination, and herein we describe ataxias that are due to lesions in the cerebellum and efferent or afferent connections. Cerebellar ataxias may be subdivided into three categories: acquired, nondegenerative ataxias; nonhereditary, degenerative ataxias; and hereditary ataxias. Hereditary ataxias can be further divided by mechanism of inheritance into those that are autosomal dominant, autosomal recessive, X-linked, and due to mitochondrial mutations.
The first autosomal recessive (AR) ataxias were described by Friedreich in the 1860s with clinical features including areflexia. In the early 1900s, cases that varied slightly from Friedreich ataxias (FRDA) were classified as atypical FRDA. Nosology was primarily based on pathologic features. Patients with markedly different clinical features might be diagnosed with “Marie” ataxia (retained reflexes and later onset than FRDA) or “Menzel” ataxia (olivopontocerebellar atrophy [OPCA] in autosomal dominant [AD] ataxia). Often, olivopontocerebellar atrophy was the term used for any non-FRDA cases as well as sporadic, late-onset ataxias. It was not until the later 20th century that Harding introduced firm clinical classification schema for hereditary ataxias. With the subsequent development of molecular genetics, loci for AR, AD, X-linked, and mitochondrial DNA mutations were discovered and added another level to classification. However, in populationbased studies, 33% to 92% of families with AD ataxias and 40% to 46% of families with AR ataxias remained without genetic diagnoses after systematic testing.
Prevalence estimates of ataxia depend on whether a clinical or genetic definition is proposed. Even when considering the rubric of clinical ataxia, worldwide prevalence is highly variable and difficult to determine because of region-specific genetic population effects, regional differences in testing and diagnosis, and limited reports from some countries. AD ataxias are the most prevalent hereditary ataxias, with a range of 0.0 to 5.6 per 100,000 and an average of 2.7 cases per 100,000. Spinocerebellar ataxia type 3 (SCA3)/Machado-Joseph disease is the most common AD ataxia, followed by SCA2 and SCA6. The prevalence of AR ataxias ranges from 0.0 to 7.2 per 100,000 with an average of 3.3 per 10,000. Among AR ataxias, Friedreich ataxia is the most frequent followed by ataxia with oculomotor apraxia or ataxia-telangiectasia.
This chapter will focus primarily on the hereditary ataxias, although the acquired ataxias will be covered in brief.
ACQUIRED ATAXIAS
Acquired etiologies of ataxia should be sought in all cases that are not clearly hereditary. Treatment for acquired ataxias is highly directed by etiology, and therefore etiologies of sporadic-appearing ataxias should be interrogated. Ataxia may be stable, progressive, or intermittent. The differential can be considered relative to rapidity of onset and includes exogenous or endogenous causes.
Acute-onset ataxia is more likely to be due to vascular disease, trauma, toxins (such as alcohol, toluene), multiple sclerosis and other demyelinating diseases, thiamine deficiency, cerebellitis (especially in children), and primary/metastatic tumor or paraneoplastic disease. It may be subacute or chronic, including due to tumor as well as paraneoplastic cerebellar degeneration (especially associated with ovary, breast, or lung neoplasm), thyroid disease, other immune-related diseases (including steroid-responsive encephalopathy thyroiditis), anti-glutamic acid decarboxylase (anti-GAD) ataxia, gluten enteropathy, vitamin E deficiency (which may be secondary to a malabsorption syndrome), toxins (including alcohol, mercury, and medications such as phenytoin), infections (including prion disease, HIV, and Whipple), leptomeningeal metastasis, vitamin B12 deficiency, and multiple system atrophy (a prominent cause of sporadic ataxia in adults associated with alpha-synuclein deposition in the pathognomonic glial cytoplasmic inclusions). In children with acquired ataxia, special concern must be given to intoxication (especially antiepileptics, lead, and alcohol), infectious or postinfectious cerebellitis (often attributable to enteroviral, picornavirus, or Epstein-Barr virus [EBV]), tumor, vascular disease, brain stem encephalitis, migraine, and hypothyroidism.
The first step in assessment for all ataxias should include neuroimaging with magnetic resonance imaging (MRI) to evaluate the cerebellum as well as additional structures and to determine the extent and etiology of cerebellar and noncerebellar disease. If acquired ataxias are not consistent with vascular, traumatic, or demyelinating disease, additional evaluation includes assessment of thyroid function, vitamin E and B 1, anti-GAD antibodies, and paraneoplastic antibodies. If suspicion of paraneoplastic etiology is present, additional work-up for assessment of a primary tumor should be considered, even in the absence of paraneoplastic antibodies. Most patients with gluten-related neurologic disease do not have associated gastrointestinal symptoms; therefore, assessment for gluten-related ataxia in an individual includes testing anti-gliadin immunoglobulin (Ig) A and IgG, antitransglutaminase-2 (anti-TG-2) and, if possible, TG-6 antibodies.
HEREDITARY ATAXIAS
Hereditary ataxias are generally progressive, although there is a subgroup of episodic hereditary ataxias, which is separately discussed.
The hereditary ataxias comprise heterogeneous disorders that share three features: ataxia, pathology involving the cerebellum or its connections, and heritability. The pathology usually affects more than the cerebellum, including also the posterior columns, pyramidal tracts, pontine nuclei, and basal ganglia, with corresponding additional neurologic signs. Clinical features may include ataxic gait and arm movements, as well as dysarthria, nystagmus, and signs of neuropathy. Within a family, clinical and pathologic features may differ and the heterogeneity creates problems for classification. Because the phenotypic range of hereditary ataxias is broad, with some family members demonstrating ataxia and other different movement disorders or parts of a syndrome— such as mental retardation in a child in proband with fragile X tremor ataxia syndrome (FXTAS)—determination of family history should query for symptoms or diagnosis of chorea, dystonia, parkinsonism, tremor, mental retardation, neuropathy, epilepsy, visual loss, diabetes, and deafness.
Ataxia is often classified based on mode of inheritance, with broad separation between the autosomal dominant cerebellar ataxias (ADCAs), the AR ataxias, and those that are X-linked and mitochondrial. However, the mode of inheritance is not always clear, owing to variable penetrance, anticipation, new mutations, small family sizes, and nonpaternity. Hereditary ataxias should be considered in apparently sporadic cases without known etiology as well. Although cases with parent-child transmission are either dominant or (if maternally inherited) mitochondrial, those with only an affected sibling may be recessive, dominant, or mitochondrial.
AR ataxias are often of early onset, and dominant ataxias are of later onset. However, as many of one-third of individuals with FRDA, the most common recessive ataxia, may have late-onset disease, among the common ADCAs, especially SCA7, but also SCA1-3, 8, and 13 may begin in childhood or even infancy. Dominant ataxias are more often associated with DNA trinucleotide repeats, but FRDA is also a trinucleotide repeat disorder. Whereas the dominant ataxias are usually believed to be due to toxic gain-of-function events, it is believed that AR ataxias are due to decreased translation and loss of functional protein. Both dominant and recessive ataxias may show cerebellar and extracerebellar neurologic features; however, nonneurologic manifestations, such as cardiomyopathy and diabetes (FRDA) and immunodeficiency (ataxia-telangiectasia [AT]), are more frequent in the recessive forms.
AUTOSOMAL DOMINANT ATAXIAS
Classification
In 1893, Marie applied the term hereditary cerebellar ataxia to syndromes that differed from Friedreich ataxia in their later-onset autosomal dominant inheritance, hyperactive tendon reflexes, and, frequently, ophthalmoplegia. Classification of ADCAs has been the subject of controversy since this time because nosology was based on pathology with poor clinical-pathologic correlation even within a single family. Harding challenged these confusing pathology-based schemes, lumping ADCAs, and then dividing them into clinical groups. With the mapping and cloning of autosomal dominant ataxia genes, emphasis has shifted to a genetic classification, incorporating clinical features when possible. A broad separation exists between those disorders that are chronic and progressive (the spinocerebellar ataxias, the SCAs) and those with primarily episodic appearance of ataxia (the episodic ataxias). Registration of SCA genes with the Human Genome Organization (HUGO) has led to a sequential numbering system of autosomal SCA loci, with 33 SCA loci and 21 known genes (Table 79.1). However, the numbering is based on the temporal order when SCA numbers were assigned and does not have clinical or pathologic significance. SCAs may be further subclassified into genetic groups (polyglutamine cytosine-adenine-guanine [CAG] repeat disorders, noncoding repeat expansions, and others), although the SCAs show tremendous clinical overlap. Nonetheless, for some SCAs, there are characteristic features which, when present, may be highly suggestive of a particular SCA. For example, seizures are prominent in SCA10, retinopathy in SCA7, and later age of onset and slower progression in SCA6 (see Table 79.1).
Epidemiology
Worldwide, ADCAs occur with a frequency of 1 to 5:100,000. Frequencies of specific SCAs vary by geographic region and this is attributed to founder effects in the populations. The most common ADCA worldwide is SCA3 (21%), then SCA2 and SCA6 (15% each), SCA1 (6%) and SCA7 (2%), and SCA8 (2-5%). The United States frequency pattern is very similar to that worldwide and SCA13 and SCA17 are also seen (less frequently than SCA8). SCA2 is common in Koreans. SCA3 is more common in Portugal, Japan, and Germany than in the United Kingdom. Dentatorubral-pallidoluysian atrophy (DRPLA) accounts for 20% of autosomal dominant SCA in Japan but is uncommon in the United States, where most cases are of African-American origin. SCA12 is common in eastern India but rare elsewhere.
Etiologic and Genetic Features
Although some distinct features can be discerned, most SCAs have many characteristics in common, and classification is complicated by intra- and interfamilial variation. Symptoms usually begin in early- or mid-adult years, but the age at onset varies from childhood to the eighth decade (see Table 79.1). The first and generally most prominent sign is gait ataxia, occasionally starting with sudden falls. Limb ataxia and dysarthria are also early symptoms. Hyperreflexia may be present initially, but tendon reflexes may later be depressed, and vibration and proprioception may be lost. Eye signs include nystagmus, slow saccades, and abnormal pursuit. Dementia, dystonia, parkinsonism, tremor, fasciculations, neuropathy, and distal wasting may occur, although the frequency of these features differs among the various SCAs. Anticipation and potentiation, earlier onset, and more severe symptoms in succeeding generations are observed in most of the SCAs (most dramatically in SCA7 and DRPLA but not in SCA6), and the majority are severely disabled 10 to 20 years after symptom onset (see Table 79.1). Some advocate classification of the ADCA by pathogenesis in those with known genes, dividing into those caused by (1) unstable CAG trinucleotide repeats in the protein-coding region leading many (poly) glutamine repeats (these include SCA1, 2, 3, 6, 7, and 17 and DRPLA); (2) noncoding repeat expansions (SCA8, 10, 12, 31, and 36); and (3) those caused by more traditional genetic mechanisms, including single gene deletions (SCA15 and 16), duplications (SCA20), and point mutations (SCA5, 11, 13, 14, 23, 27, 28, and 35). Among this last class are genes associated with glutamate signaling (SCA5), tau regulation (SCA11 and 27), ion channel functions (SCA13 and 14), mitochondrial activity (SCA28), and calcium signaling (SCA15/16). Whereas ADCAs are generally progressive, the subgroup of episodic ataxias is predominantly intermittent. It is associated with mutations in ion channel genes (EA1, 2, and 5) or signaling (glutamate, EA6) and is separately discussed, although there is overlap with the other ADCAs, as SCA6 is due to CAG repeats in the calcium channel gene CACNA1A. In SCAs with repeat expansions, paternal and maternal transmissions differ, and in all but SCA8, there is a greater tendency for an increase in repeat size in paternally transmitted disease chromosomes. As a result, anticipation is more pronounced in paternally transmitted disease. In SCA8, most expansions occur during maternal transmission.
Coding CAG and Polyglutamine Disorders (Spinocerebellar Ataxia Types 1, 2, 3, 6, 7, and 17 and Dentatorubral-Pallidoluysian Atrophy)
SCA1, SCA2, SCA3, SCA6, and SCA7 are the most frequent etiologies of ADCAs in families worldwide, together accounting for
50% to 60%. As in other dominant disorders with trinucleotide expansions (e.g., Huntington disease, DRPLA), there is generally an inverse relationship between repeat size and age at onset, with a threshold of expanded alleles needed for disease. However, in some of these there is an intermediate range of alleles, whereby the upper limit of normal overlaps with the lower range of abnormal repeats. These are now separated into “mutable normal” alleles where they are not disease causing but with transmission expand to cause disease and “reduced penetrance” alleles that may or may not cause disease. Another feature of the trinucleotide expansion disorders is meiotic instability and anticipation. In a parent-child transmission, the size of the repeat may change, either expanding or contracting; with expansion, there may be earlier onset or worse severity in subsequent generations (anticipation).
TABLE 79.1 Autosomal Dominant Ataxias
Disorder
Gene (Mutation Type/Locus)
Gene Product
Phenotype: Age of Onset (Years, Range) Some Typical Featuresa
The CAG expansions result in an expanded polyglutamine tract because CAG codes for glutamine. Unlike the FRDA triplet expansion in the recessive Friedreich ataxia, which causes disease by inducing frataxin deficiency, the dominant SCA triplet expansions cause disease by altering the protein, a toxic gain of function. Polyglutamine protein inclusions are postulated due to impaired protein clearance and transcriptional dysregulation. As each polyglutamine disorder has distinctive clinical-pathologic features, some other feature, in addition to the polyglutamine, must play a role.
SPINOCEREBELLAR ATAXIA TYPE 1
The first ADCA locus, SCA1, was mapped to the short arm of chromosome 6 in 1974, and in 1993, the SCA1 mutation was identified as due to a trinucleotide (CAG) repeat expansion. The expansion was specifically sought because of the known anticipation in SCA1 families and the earlier identification of expanded trinucleotide repeats and anticipation in Huntington disease. The protein encoded by SCA1 is called ataxin-1 (ATXN1), a ubiquitously expressed protein of unknown function. Mutated ATXN1 accumulates in the nucleus into aggregates, termed nuclear inclusions. These inclusions include ubiquitin, chaperones, and proteasomal subunits that are important for protein refolding and degradation, and abnormal protein clearance thus may mediate SCA1 pathogenicity.
Different trinucleotide repeats, those with cytosine-adenine-thymine (CAT), serve to stabilize the polyglutamine repeat from expanding. Normal SCA1 alleles have 6 to 44 CAG repeats, and the repeat configuration is interrupted by one to three CAT repeats when the allele contains 21 or more repeats. Abnormal alleles have 39 or more repeats without the CAT interruption. Mutable normal (intermediate) alleles are those with 36 to 38 CAG repeats without the CAT interruption. Intermediate alleles appear to have no associated clinical signs but on transmission to offspring can expand to the abnormal range. As with other polyglutamine disorders, the repeat size is overall associated with earlier age of onset and severity of disease, but approximately half of the variance in age at onset is not fully explained by repeat size alone; therefore, additional mechanisms are involved.
The prevalence of SCA1 is estimated at 1 to 2 per 100,000, varying in different populations. It is estimated to be responsible for 6% of ADCAs in North America, approximately 30% in Italy, England, and Serbia, and 40% in South Africa. SCA1 rarely accounts for ataxia in singleton or apparently recessive cases.
Typically, SCA1 starts in the third to fourth decade, but the range at onset is 6 years of age to late adulthood. Gait ataxia predominates and is often the first sign, usually with mild dysarthria, hypermetric saccades, nystagmus, and hyperreflexia. With progression, nystagmus may disappear and saccadic abnormalities and ophthalmoparesis (particularly upgaze) develop. Worsening limb, gait, and speech ataxia evolve. Hypotonia with decreased tendon reflexes and sensory loss are common later. Although mild dysphagia may occur early, bulbar manifestations including lingual atrophy, fasciculations, and severe dysphagia usually present late in the disease. Optic atrophy, dementia, personality change, dystonia, and chorea are less common. Maculopathy, more common in SCA7, has also been reported. Classically, SCA1 is more rapidly progressive than other SCAs, with progression to death in 10 to 30 years and early-onset disease more rapidly progressive. Lateonset disease may be restricted to a pure cerebellar disorder, as is seen in SCA6.
The pathology includes neuronal loss in the cerebellum, brain stem, spinocerebellar tracts, and dorsal columns with rare involvement of the substantia nigra and basal ganglia. Purkinje cell loss and severe neuronal degeneration in the inferior olive are seen; degeneration is also seen in the cranial nerve nuclei, restiform body, brachium conjunctivum, dorsal and ventral spinocerebellar tracts, posterior columns, and, rarely, the anterior horn cells. MRI shows atrophy of the brachia pontis and anterior lobe of the cerebellum and enlargement of the fourth ventricle, and spinal cord atrophy may be present.
SPINOCEREBELLAR ATAXIA TYPE 2
Mapped in ataxic patients from the Holguin province of Cuba who descended from an Iberian founder, SCA2 families were subsequently found in Italy, Germany, French Canada, Tunisia, and Japan. The SCA2 gene encodes the protein ataxin-2.
Normal individuals have 31 or fewer CAG repeats (with most containing 22), with 32 repeats of uncertain significance and CAG expansions of 33 or more associated with disease. Repeat length closely correlates with age at onset and severity. SCA2 may have marked anticipation, instability, and expansions. Large expansions over 200 and homozygosity are associated with retinitis pigmentosa, myoclonic encephalopathy, and early-onset parkinsonism. Intermediate length expansions may increase the risk of amyotrophic lateral sclerosis (ALS) and the atypical parkinsonism, progressive supranuclear palsy (PSP), and repeats of 33 or more or with a preserved CAA interruption may manifest as ALS or levodopa-responsive parkinsonism. The function of ataxin-2, the protein encoded by SCA2, is not known, but in normal and SCA2 brains, it is localized in the cytoplasm of neurons, especially Purkinje cells. Immunocytochemical studies suggest that the protein is associated with endoplasmic reticulum and may be involved in processing of mRNA and/or regulation of translation, and elevated repeats lead to aggregation of disease protein. Further, ataxin-2 knockout models suggest that it may play a role in modification of other neurodegenerative diseases, including not only ALS but SCA1 and 3 as well.
SCA2 is a relatively frequent cause of ADCA worldwide, ranging from 14% to 18% in German and American ADCA families, to 37% to 47% in Italian and English families, and more than 30% in ADCA families from eastern India. Rarely, it is found in families with apparent recessive inheritance (i.e., siblings but not parents affected) or in sporadic cases, and some of this may be attributed to the tremendous anticipation whereby the child with markedly more repeats presents prior to the parent with fewer, albeit pathologic, repeats.
SCA2 usually begins in the third to fourth decade, but onset varies from infancy to the seventh decade. The most common clinical features are progressive gait and limb ataxia and dysarthria (Video 79.1). SCA2 is often described as a cerebellar-plus disorder, as other accompanying features are common and include depressed or absent tendon reflexes, slow saccades, kinetic or postural arm tremor, fasciculations, ophthalmoparesis, vibratory and position sensory loss, and sleep disturbances. Chorea and dystonia have been reported in 38% of cases and dementia in 37%. Less common features are leg cramps and leg hyperreflexia. Although levodoparesponsive parkinsonism is classically associated with SCA3, it may be present in SCA2 as well. Nystagmus is an initial feature that tends to disappear as slow saccades emerge. Although other SCA subtypes include these features, patients with SCA2 are most likely to have slow saccades and hyporeflexia. Many show electrophysiologic evidence of axonal neuropathy with severe involvement of sensory fibers. The highly variable phenotype occasionally seems to “breed true” in families (e.g., kindreds with dementia and extrapyramidal signs or with moderate ataxia, facial fasciculations, prominent eye signs that include lid lag, and retinitis). Abnormal motor control with periodic leg movements during sleep and rapid eye movement (REM) sleep without atonia are common.
Pathology, like clinical signs, is variable. Usually, there is severe neuronal loss in the inferior olive, pons, and cerebellum (OPCA). However, there may also be degeneration of the substantia nigra, dorsal columns, and anterior horn cells. Degeneration is rarely restricted to the cerebellum.
As with other SCAs, because there are overlapping clinical features, molecular genetic testing is necessary to confirm the diagnosis.
SPINOCEREBELLAR ATAXIA TYPE 3/MACHADO-JOSEPH DISEASE
Machado-Joseph disease (MJD) was first described in families of Azorean Portuguese descent, also seen in German, Dutch, African-American, and Japanese families, and eventually linked to chromosome 14q24.3-q32. Subsequent linkage to the same region was found in French families that were clinically similar to SCA1 or SCA2, and the locus was numbered SCA3. Because these French families were not of Azorean descent, and because there were several clinical differences (lack of dystonia and facial fasciculations), it was uncertain whether MJD and SCA3 were owing to different genes, different mutations in the same gene, or the varying phenotypic expressions of the same mutation in individuals with different ancestry. In 1994, an expanded and unstable CAG repeat was found in the coding region of the MJD gene and all 14q-linked families have the same unstable CAG repeat within the SCA3/MJD gene, so that now SCA3 and MJD are viewed as a single genetic disorder with a wide clinical spectrum. SCA3 is the most common ADCA worldwide. As with the other ADCA genes, there may be intrafamilial genetic modifiers (including differences within the SCA3/MJD gene) that influence the phenotype.
The normal repeat number is up to 43, and disease alleles in affected individuals range from 52 to 89 repeats. Intermediate allele size is between 48 and 54 repeats, is associated with meiotic instability and pathologic expansion in subsequent generations, and infrequently may manifest with restless legs syndrome, dysautonomia, and/or polyneuropathy. As in other CAG repeat diseases, there is a strong inverse correlation between the length of the repeat and age at onset, and there is instability in paternal meioses. Some, but not all, homozygous SCA3 individuals have early-onset severe disease, suggesting a gene dosage effect.
The SCA3/MJD gene encodes ataxin-3, a protein not related to ataxin-1 or ataxin-2. It binds and cleaves ubiquitin chains, suggesting that it may be a mixed linkage, ubiquitin chain-editing or regulatory enzyme linked to quality control and endoplasmic reticulum-associated protein degradation. It is ubiquitously expressed in the cytoplasm of cell bodies and processes. In SCA3/MJD brain, there is aberrant nuclear localization and accumulation of ubiquitinated nuclear inclusions. The sites and burden of brain degradation in SCA3 is similar to SCA2.
Common signs, regardless of age at onset, include limb and gait ataxia, dysarthria, and progressive ophthalmoplegia. Findings that are more dependent on age at onset include pyramidal signs, dystonia and rigidity, amyotrophy, facial and lingual fasciculations, and lid retraction with bulging eyes. Four clinical subclasses have been proposed:
Adolescent or young adult onset: rapidly progressive with spasticity, rigidity, bradykinesia, weakness, dystonia, and ataxia
Mid-adult onset (ages 30 to 50 years): moderate progression of ataxia
Late-adult onset (ages 40 to 70 years): slower progression of ataxia, prominent peripheral nerve signs, and few extrapyramidal findings
Adult onset: parkinsonism and peripheral neuropathy
The pathology had been considered distinct with primarily spinopontine atrophy and involvement of pontine nuclei, spinocerebellar tracts, Clarke column, anterior horn cells, substantia nigra, and basal ganglia; the inferior olives and cerebellar cortex were thought to be always spared. With mutation screening, however, it is now evident that the olives and cerebellar cortex may be involved.
SCA3 is the most common cause of ADCA in many but not all populations. In the United States, about 21% of ADCA families have SCA3; in a study of mixed populations, 41% were SCA3, but this dropped to 17% when Portuguese families were excluded. SCA3 is common in Germany (accounting for 50% of ADCA cases), China, and Japan but uncommon in England and rare in Italy (Figs. 79.1 and 79.2).
SPINOCEREBELLAR ATAXIA TYPE 6
The SCA6 gene maps to chromosome 19p13 and encodes for an α1A voltage-dependent calcium channel subunit (CACNA1A). It differs from other polyglutamine SCAs in the following: (1) Pathology is associated with a lower number of CAG repeats; (2) repeat is stable during transmission and anticipation is generally not observed; (3) there is a later onset, less severely progressive course, and the disorder tends to be more purely cerebellar; and (4) it is allelic with other generally nonprogressive channelopathies. There are three distinct phenotypes associated with different CACNA1A mutations. The SCA6 symbol is reserved for an adult-onset cerebellar syndrome with CAG repeat expansions. SCA6 CAG repeats are 20 to 33, with an average disease-causing length of 22. Normal expansions are 4 to 18, and 19 repeats are considered intermediate.
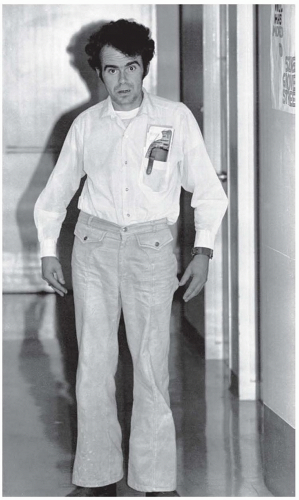
FIGURE 79.1 Patient JM of the Joseph family who, at age 38 years, shows dystonic posturing of his head, arms, trunk, and legs in association with prominent spasticity of his extremities. He has been symptomatic for 12 years. (From Rosenberg RN, Nyhan WL, Coutinho P, et al. Joseph’s disease: an autosomal dominant neurological disease in the Portuguese of the United States and the Azores Islands. Adv Neurol. 1978;21:33-57.)
The two other phenotypes associated with CACNA1A mutations are familial hemiplegic migraine (FHM) and episodic ataxia type 2 (EA2). EA2 is caused by CACNA1A mutations that predict protein truncation, abnormal splicing, or, rarely, missense mutations, and about 50% of FHM is associated with CACNA1A missense mutations. In addition, a CACNA1A missense mutation, G293R, causes a more severe SCA6-like phenotype. Although most families “breed true” as SCA6, FHM, or EA2, phenotypic overlap may occur. SCA6 patients may also have episodes of ataxia. One family with CAG expansions had members with episodic ataxia and others with progressive ataxia and another with EA2 had members with hemiplegia or migraine during episodes of ataxia. The correlation between number of SCA6 repeats and age at onset is quite loose; 22 repeats, the most common expansion, is associated with range of age at onset, even within sibships. Like MJD, the phenotype is more severe in homozygous individuals.
FIGURE 79.2 A 74-year-old man and grandson of the Joseph proband showed progressive disease for 12 years with truncal ataxia, cerebellar dysarthria, areflexia, distal sensory deficits, and distal atrophy. The degree of atrophy of the intrinsic hand muscles can be seen. Thus, he manifests a neurologic syndrome of late onset and, as a direct descendant of Antone Joseph, he suggests the possibility of a wide spectrum of disease. (From Rosenberg RN, Nyhan WL, Coutinho P, et al. Joseph’s disease: an autosomal dominant neurological disease in the Portuguese of the United States and the Azores Islands. Adv Neurol. 1978;21:33-57.)
The molecular basis of disease is unknown, and thus far, studies suggest that expanded CAG repeats do not affect the functioning of the voltage-gated calcium channels but rather reflect a gain of function of the protein, although this remains an area of active research.
The clinical picture of SCA6 is fairly uniform. The average age at onset is somewhat older than other SCAs, about 45 to 50 years (range, 20 to 75 years). The first symptom is usually unsteady gait. Dysarthria, leg cramps, and diplopia can also be early symptoms. Occasionally, patients describe positional vertigo or nausea. Cerebellar signs include gait and limb ataxia (especially leg), cerebellar dysarthria, saccadic pursuit, and dysmetric saccades. Horizontal and downbeat nystagmus (most prominent on lateral gaze) are common eye signs, but very slow saccades are not observed. Noncerebellar signs occur with less frequency and usually less clinical impact than in other SCA disorders but include hyperreflexia, decreased vibration and position sense, impaired upgaze, and parkinsonism. Onset of ataxia may be episodic or apoplectic and resembles EA2 with attacks of unsteadiness, vertigo, and dysarthria that last for hours; between attacks, there are few if any symptoms or signs. The attacks may occur for years before progressive cerebellar signs emerge.
The course is slowly progressive, the least progressive of the SCAs and generally does not shorten life span. After 10 to 15 years, most affected individuals are no longer able to walk without assistance. MRI shows cerebellar atrophy but little brain stem or cortical atrophy. Pathologically, there is cerebellar atrophy with loss of Purkinje and granule cells and limited involvement of the inferior olives.
In the United States and Germany, SCA6 accounts for 10% to 15% of ADCA families. It is more common in Japan (30%) and is uncommon in France, where only 1% of ADCA families harbor the mutation. Five percent to 6% of sporadic ataxia patients demonstrate SCA6 expansions. Some are new mutations, but it is also likely that some appear sporadic because of the late age at onset and relatively indolent course.
SPINOCEREBELLAR ATAXIA TYPE 7
SCA7 differs from other forms of ADCA by the associated severe retinal photoreceptor degeneration producing cone-rod dystrophy and is notable for unstable repeat length during meiosis. It is a result of the expansion of a coding sequence CAG repeat in ataxin-7, an integral component of the transcription coactivator complex involved in regulation of transcription. Normal alleles have up to 29 repeats. Abnormal alleles have from 36 to more than 450 repeats. Intermediate repeats are between 30 and 35. Alleles in this range are considered to be unstable, producing an increased risk of having a child with an abnormal repeat length but are not convincingly associated with a phenotype. Dramatic examples of anticipation, especially with paternal transmission, are due to repeat instability, which exceeds any other CAG repeat SCA, and is related to age at onset, rate of progression, and clinical signs.
SCA7 age at onset ranges from infancy to the seventh decade and averages around 30 years. The course varies with age at onset. A severe infantile form occurs with large expansions (>200) that are paternally inherited. These infants have hypotonia, dysphagia, visual loss, cerebellar and cerebral atrophy, and congestive heart failure with cardiac anomalies. This differs from childhood and adult forms, which are marked by early visual loss, moderately progressive limb and gait ataxia, dysarthria, ophthalmoparesis, and Babinski signs. In late-onset cases (fourth to sixth decade), ataxia may occur in isolation or it may precede visual symptoms (see Table 79.1). Affected individuals all have abnormal yellow-blue color discrimination (which in the mildest forms may be asymptomatic), and clinically, there is often optic disc pallor with granular and atrophic changes in the macula.
Degeneration affects the cerebellum, basis pontis, inferior olive, and retinal ganglion cells. Neuronal intranuclear inclusions containing the expanded polyglutamine tract are found in many brain regions, most frequently in the inferior olive. SCA7 accounts for almost all families with both ADCA and retinal degeneration and about 5% of all ADCA families.
SPINOCEREBELLAR ATAXIA TYPE 17
Initially described in a Japanese patient with childhood-onset ataxia and no family history, SCA17 has now been reported in Japanese and European kindreds. Age at onset ranges from 19 to 48 years, starting with gait ataxia and dementia. Psychiatric features sometimes precede the motor disorder. Limb ataxia, hyperreflexia, chorea, dystonia, myoclonus, parkinsonism (including tremor, bradykinesia, postural instability, and rigidity, sometimes mimicking MSA-C), as well as epilepsy have also been reported. MRI is notable for both cerebral and cerebellar atrophy. SCA17 is secondary to a CAG repeat expansion in the TATA-binding protein (TBG) gene, a transcription-initiating factor (TFIID). Normal repeat length is 29 to 42, and patients have 44 to 63 CAG repeats. Similar to SCA6, repeats are generally stable in subsequent generations. Neuropathology demonstrates Purkinje cell loss and intranuclear inclusions with polyglutamine expansions.
DENTATORUBRAL-PALLIDOLUYSIAN ATROPHY
DRPLA is most common in Japan where it constitutes 10% to 20% of ADCA families. Rare cases have been described in other groups. The pathology involves the dentate, red nucleus, subthalamic nucleus, and the external globus pallidus; the posterior columns may be involved. The phenotype includes ataxia and dementia but varies in other features depending on age at onset. Early-onset cases (before age 20 years) tend to show severe and rapid progression of myoclonus, epilepsy, and cognitive decline, whereas later onset cases display ataxia, chorea, dementia, and psychiatric problems (resembling Huntington disease; see Table 79.1). Anticipation is evident, and paternal transmission is associated with more severe early-onset disease. One clinical variant, the Haw River syndrome, was described in an African-American family in North Carolina. This variant includes all the aforementioned symptoms except for myoclonic seizures, and additional features include basal ganglia calcification, neuroaxonal dystrophy, and demyelination of the central white matter. MRI may show atrophy of the cerebral cortex, cerebellum, and pontomesencephalic tegmentum, with high signal in white matter of the cerebrum and brain stem.
The disorder is a result of an expansion of a CAG repeat in the DRPLA gene, which maps to chromosome 12p. There is an inverse relationship between repeat size and age at onset; normal subjects have up to 35 repeats and disease alleles have 48 or more (see Table 79.1). The gene is expressed in all tissues, including brain. The DRPLA gene product, atrophin-1, is found in neuronal cytoplasm. Ubiquinated intranuclear inclusions are seen in neurons and to a lesser extent in glia. The neuronal inclusions are concentrated in the striatum, pontine nuclei, inferior olive, cerebellar cortex, and dentate.
Spinocerebellar Ataxias due to Noncoding Repeat Expansions (Spinocerebellar Ataxia Types 8, 10, 12, 31, and 36)
In contrast to the polyglutamine disorders, these SCAs are due to repeat expansions, usually trinucleotide, pentanucleotide, or hexanucleotide, which are transcribed to RNA but are not translated into protein.
SPINOCEREBELLAR ATAXIA TYPE 8
SCA8 has a slowly progressive course that begins at a mean of 39 years (range 1 to 65 years). The common initial findings include limb and gait ataxia and dysarthria and, compared to other SCAs, severe scanning dysarthria, truncal titubation, and leg ataxia are more common. Severely affected individuals are not able to walk by the fourth decade. Hyperreflexia, Babinski signs with spasticity, and ophthalmoplegia may also occur.
SCA8 is unique among the ataxia trinucleotide repeat disorders for several reasons: (1) The trinucleotide repeat is a cytosine-thymine-guanine (CTG) repeat rather than a CAG repeat, (2) the repeat length does not necessarily correlate with severity, (3) abnormal allele length has been reported in other ataxias as well as normal controls, and (4) allele expansion occurs with maternal transmission and contraction with paternal transmission. It is similar to SCA12 (a CAG trinucleotide repeat) but differs from other trinucleotide repeat disorders in that the product is a noncoding RNA. Abnormal CTG expansions (>44 repeats) have been reported in healthy and disease controls. The SCA8 transcript may downregulate the adjacent gene Kelch-like 1 (KLHL1), leading to neurodegeneration. However, initial studies with transgenic mice suggest that CTG expansions produce an ataxic phenotype.
SPINOCEREBELLAR ATAXIA TYPE 10
SCA10 is caused by a large ATTCT pentanucleotide repeat expansion in intron 9 of ataxin-10, a new type of dynamic repeat expansion. Although the normal repeat range is 10 to 22 alleles, affected individuals have 800 to 4,500 repeats. The expanded repeat alleles are unstable with paternal transmission, and there is an inverse correlation between the repeat number and age at onset. An association between ataxia or seizure phenotype and allele size has not been established.
In 1999, two independent groups mapped this locus to chromosome 22q. The phenotype is marked by pure cerebellar signs and seizures. Most families are of Mexican or Brazilian ancestry suggesting a common, possibly Native American, founder population. Age at onset ranges from 12 to 48 years, with evidence of anticipation. There is slowly progressive ataxia with eventual difficulty sitting. Scanning dysarthria, dyscoordination of oral muscles, upper limb incoordination, and abnormal tracking eye movements also develop in most patients. Although seizures may be infrequently associated with SCA2 and SCA17, they are a prominent feature in SCA10: between 20% and 100% of patients have recurrent partial complex and generalized motor seizures. Seizures usually start after the gait ataxia and are well controlled with anticonvulsants. Mild cognitive disorders, mood disorders, mild pyramidal signs, behavioral disturbances, and peripheral neuropathy may occur. Furthermore, nonneurologic features of hepatic failure, anemia, and/or thrombocytopenia were reported in one family. MRI demonstrates progressive pancerebellar atrophy, and interictal electroencephalogram shows evidence of cortical dysfunction with or without focal epileptiform discharges in some.
Only gold members can continue reading. Log In or Register to continue