Acquired immunodeficiency syndrome (AIDS) is the most devastating pandemic of the 20th and early 21st centuries. It was first recognized in 1981 through a growing number of reports of rare opportunistic infections, including Pneumocystis carinii pneumonia (PCP), and malignancies, such as Kaposi sarcoma, occurring in previously healthy gay men. Similar cases were discovered in intravenous (IV) drug users, and in 1982, the Centers for Disease Control and Prevention (CDC) proposed epidemiologic surveillance criteria. In 1983, human immunodeficiency virus (HIV) type 1 was isolated from human peripheral blood lymphocytes, and shortly thereafter, this retrovirus was established as the cause of AIDS. As the worldwide magnitude of the HIV pandemic became clear, the pace of research grew. The virus was sequenced and its structure elucidated by x-ray crystallography. The life cycle of the HIV, with the discovery of binding to the CD4 glycoprotein receptor, leading to the immune dysregulation was discovered soon after initial viral identification. Further understanding of the mechanisms of human infection and pathogenesis and development of successful drug therapies occurred. Central nervous system (CNS) complications due to infection by HIV-1 were first described early in the epidemic, when severe neurocognitive disease attributable to the virus was common in individuals with profound immunodeficiency.
CLASSIFICATION OF HIV DISEASE
In 1986, the CDC proposed staging criteria for HIV infection. These were modified in 1987 to include HIV-associated dementia and myelopathy among the 23 AIDS-defining illnesses. Revisions, in 1993, added three laboratory categories that are stratified by CD4 cell numbers and three clinical categories (Table 67.1).
AIDS-defining illnesses were expanded to include positive HIV serology and pulmonary tuberculosis (TB), recurrent bacterial pneumonia, invasive cervical carcinoma, or a CD4 lymphocyte count less than 200 cells/mm3. These revisions define the end stage of HIV infection and clarify the relationship of specific clinical syndromes, especially those affecting the nervous system that are not themselves diagnostic of AIDS, to advanced immunosuppression. In contrast to the CDC system, the World Health Organization (WHO) Clinical Staging and Disease Classification System revised in 2006 can be used readily in resource-constrained settings without access to CD4 cell count measurements or other diagnostic and laboratory testing methods (Table 67.2).
The WHO system classified HIV disease on the basis of clinical manifestations that can be recognized and treated by clinicians in diverse settings and by clinicians with varying levels of HIV expertise and training. This classification system guides medical management of HIV-infected persons. CD4 lymphocyte count levels and viral load assays have mostly supplanted staging criteria for decisions about antiretroviral therapy. Staging is still useful for prognosis and decisions about opportunistic infection prophylaxis and identifying patients most at risk for opportunistic infections and malignancy.
EPIDEMIOLOGY
HIV infection is still an enduring pandemic affecting virtually all population groups and countries. According to the 2013 UNAIDS report, in 2012, there were 35 million people worldwide living with HIV infection. Among these HIV-positive individuals, 25 million (71%) are living in sub-Saharan Africa and 1.3 million live in North America. HIV-2 is restricted to West Africa and those countries with historical and socioeconomic ties to the region and commonly co-occurs with HIV-1. Retrospective analysis of banked blood showed that HIV was present in the United States in the 1970s. In 2013, the CDC estimated the prevalence of HIV/AIDS at 1.1 million Americans (Table 67.3). Estimates were that 16% of infected individuals were unaware of their HIV status. Cumulative deaths due to AIDS totaled 636,000, with 15,529 deaths in 2010.
In 2000, AIDS became the leading cause of death among African-American men aged 35 to 44 years and women aged 25 to 34 years. The disproportionate representation of African-American and Hispanic men is related to IV drug use: African-Americans represent approximately 12% of the U.S. population but accounted for an estimated 44% of new HIV infections in 2009. African-Americans also accounted for 44% of individuals living with HIV infection in 2009. Hispanic/Latinos represent 16% of the U.S. population but accounted for 19% of individuals living with HIV infection in 2009. Although affected by drug use, unprotected heterosexual activity has become the predominant transmission risk for minority women. There has also been a significant increase in the incidence of HIV infection among the elderly. By 2015, it is anticipated that 50% of HIV-seropositive individuals will be older than age 50 years.
TABLE 67.1 1992 Centers for Disease Control and Prevention Classification of HIV Infection
Laboratory Categories
Category 1—CD4 lymphocyte count >500 cells/mm3
Category 2—CD4 lymphocyte count from 200 through 499 cells/mm3
Category 3—CD4 lymphocyte count <200 cells/mm3
Clinical Categories
Category A—asymptomatic infection, persistent generalized lymphadenopathy, and acute primary HIV infection
Category B—symptomatic conditions not included in the CDC 1987 surveillance case definition of AIDS that are judged by a physician to be HIV related or where medical management is complicated by HIV infection (e.g., sepsis, bacterial endocarditis, pulmonary TB, cervical dysplasia or carcinoma, vulvovaginal candidiasis)
Category C—any of the 23 conditions listed in CDC 1987 case definition for AIDS
CDC, Centers for Disease Control and Prevention; TB, tuberculosis.
Adapted from United States Congress, Office of Technology Assessment. The CDC’s Case Definition of AIDS: Implications of the Proposed Revisions-Background Paper. Washington, DC: US Government Printing Office; 1992.
TABLE 67.2 World Health Organization Clinical Staging of Established HIV Infection
HIV-Associated Symptoms
WHO Clinical Stage
Asymptomatic
1
Mild symptoms
2
Advanced symptoms
3
Severe symptoms
4
Adapted from World Health Organization. WHO Case Definitions of HIV for Surveillance and Revised Clinical Staging and Immunological Classification of HIV-Related Disease in Adults and Children; 2007.
The introduction of combination antiretroviral therapy (cART) in 1996 profoundly changed HIV/AIDS epidemiology in the United States and other resource-rich countries. Since the introduction of cART, there has been a 38% decline in incident AIDS cases and a 67% decline in deaths from AIDS in the United States. Progress in some developing countries remains hampered by limited access to formal cART programs. Through the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR), UNAIDS, the WHO, as well as nongovernmental organizations and local ministries of health, there has been an increase in formal cART programs in many developing regions, with the hopes of disease stabilization in the next 5 to 10 years.
TABLE 67.3 Epidemiology of HIV/AIDS: United States and Global Data: 2012 and 2013
United States—through 2012
Adults/adolescents
1,144,500
Pediatric (<13 yr)
10,834
Total
1,155,334
Demographics (Adult)
Race
African-American
44%
Non-Hispanic white
34%
Hispanic
21%
Gender
Men
75%
Women
25%
Global—2008
Total cases through 2012
35,300,000
Sub-Saharan Africa
25,500,000
South and Southeast Asia
3,900,000
Number of new HIV infections in 2007
2,300,000
Deaths due to AIDS in 2012
1,600,000
Children with AIDS (<15 yr) in 2012
3,300,000
Adapted from Centers for Disease Control and Prevention. www.cdc.gov. 2013; 2013 World Health Statistics. World Health Organization. www.who.int.
The major routes of HIV transmission include sexual contact, mother-to-child, injection drug use with contaminated needles, and exposure to infected blood or blood products, with sexual transmission being the most common route of exposure worldwide. Worldwide, heterosexual activity is the most common mode of transmission. In the United States, homosexual activity is the most common risk behavior (45%) followed by high-risk heterosexual behavior (27%) and injection drug use (22%). The fastestgrowing populations with AIDS in the United States are women (who account for 26% of cases), African-American and Hispanic minorities, and IV drug users.
Recipients of blood products or clotting factor for hemophilia, or other coagulation/blood disorders, account for less than 1% of adult AIDS cases. In the United States, routine testing of blood products has largely eliminated this source of infection. Occupational exposure with validated transmission and seroconversion is well documented but rare. Most percutaneous or mucocutaneous exposures have been to blood or bloody fluid. Prospective studies of known exposures estimate the average risk for HIV transmission following percutaneous exposure (“needlestick”) to be approximately 0.3% and after mucous membrane exposure, 0.09%.
AIDS IN CHILDREN
This topic is discussed more fully in Chapter 147. By the end of 2012, nearly 4,500 children in North America younger than the age of 15 years were living with HIV infection. Most children are infected perinatally. Since 1992, perinatal transmission in the United States has declined sharply, from a peak of 1,000 to 2,000 cases annually to only 38 cases in 2006 resulting from successful implementation of CDC guidelines for maternal counseling, testing, and antiretroviral treatment.
Worldwide, however, perinatal transmission continues to post a large burden on worldwide incidence of HIV infection. There are an estimated 3.3 million HIV infections in children in 2012, with 260,000 new infections in 2012. Among these new infections in children, 88% of them are in sub-Saharan Africa. Perinatal infection of children depends on maternal viral load and the stage of pregnancy during which the infection is acquired. After delivery, a substantial number of children return to seronegative status.
Hallmarks of early infection include developmental delay and cognitive dysfunction, loss of previously acquired milestones, and vasculopathy that can cause stroke or hemorrhage. In Africa, some studies show no difference in neuropsychological measures and school success in HIV-positive children compared with HIV-negative controls who have similar nutritional and socioeconomic status. However, a mortality rate of 61% by age 4 years for very ill children must qualify such a comparison.
ETIOLOGY
HIV is an enveloped RNA lentivirus. It contains an RNA-dependent DNA polymerase (reverse transcriptase) that produces a provirus capable of integrating into host cell DNA. In the target cell, the virus exists in both free and integrated states.
Human HIV infection is considered a cross-species (zoonotic) infection, arising from monkeys infected with simian immunodeficiency virus (SIV) through multiple independent transmissions. Of the two recognized viral species, HIV-1 is found worldwide and is more prevalent, whereas HIV-2 is found in Western Africa and in Europe among African immigrants and their sexual partners. Sporadic cases of HIV-2 occur in the United States, but they are rare in comparison to HIV-1. A variety of evidence suggests that the AIDS pandemic most likely originated in equatorial Western Africa. HIV-1 is characterized by extensive genetic diversity and can be divided into three classes: group M (major), group O (outlier), and group N (new, non-M, and non-O). Group M is responsible for 90% of cases of HIV infection globally and is represented by nine major subtypes or clades. The HIV-1 subtypes in the United States and Europe differ from the subtypes seen elsewhere in the world. In the United States and Europe, clade B is the predominant subtype, whereas in sub-Saharan Africa, clades A, C, and D are predominant subtypes.
PATHOBIOLOGY
The primary infectious event includes breach of a mucosal barrier, enhancing viral entry. Viremia drives infection and massive depletion of CD4 T cells, particularly in the gut-associated lymphoid tissue (GALT). The immune reaction to the virus causes activation of CD8 T cells and virus-specific antibody production, which in turn promotes rebound of CD4 T cells and slowed viral replication, although importantly the mucosal lymph system does not recover to its preinfective condition. Progression of HIV is caused in part by this constant immune activation that detrimentally affects the immune system through a combination of direct loss of infected CD4 T lymphocytes and bystander cell killing. Infection of CD4 lymphocytes by HIV, mediated by viral attachment to the cell surface CD4 receptor, leads to cell death. In humans, the CD4 receptor is expressed on several cell types, including neurons and glia in the brain, but there is no evidence of viral replication in cells other than lymphocytes, macrophages, monocytes, and their derivatives. In 1996, a chemokine receptor was identified as a coreceptor that is necessary for viral entry into cells. In acute and early HIV infection, an M-tropic viral strain that prefers to replicate in macrophages with the chemokine receptor CCR5 predominates (R5 strain). In advanced infection, a T-tropic viral strain that prefers T cells with the chemokine receptor CXCR4 evolves and becomes predominant (X4 virus). Genetic variation in the chemokine receptor may affect susceptibility to HIV infection. Relative resistance to infection is observed in individuals who are homozygous for a 32 base-pair deletion in CCR5. Progression rates in AIDS may be affected by changes in the presentation of viral epitopes by infected cells to cytotoxic T lymphocytes. Accelerated progression to AIDS is associated with a single amino acid substitution in the HLA-B35 allele (HLA-B*35-Px). However, the predictive value of observations about the effect of HLA polymorphisms on disease progression might be restricted to specific populations. Primary HIV infection can be asymptomatic or, in 50% to 70% of the cases, results in an acute, self-limited mononucleosis-like illness with fever, headache, myalgia, malaise, lethargy, sore throat, lymphadenopathy, and maculopapular rash. Painful ulceration of the buccal mucosa may impede swallowing (odynophagia).
Acute infection is characterized by viremia, high viral replication rates (up to 1 million RNA molecules per milliliter), viral isolation from peripheral blood lymphocytes, and high serum levels of a viral-core antigen, p24. Cytotoxic lymphocytes and soluble factors from CD8 lymphocytes are effective in reducing viral load to a set point that differs for each individual. Despite the effective early immune response, there is almost simultaneous immune dysfunction. Neutralizing antibodies, initially immunoglobulin (Ig) M and later IgG, appear in 2 to 6 weeks, resulting in clearance of viremia and a decrease in serum p24 levels. Rarely, antibodies do not appear for several months or, exceptionally, not at all.
Adverse immunologic effects occur early and are more severe in symptomatic persons. An early absolute lymphopenia affects both CD4 helper and CD8 suppressor cells with lymphocyte hyporesponsiveness to mitogens and antigens and thrombocytopenia. Lymphocytosis, especially of CD8 lymphocytes, usually follows with inversion of the CD4/CD8 ratio. Atypical lymphocytes are sometimes seen. Early changes in the CD4/CD8 ratio are usually transient, but reversion to more normal values is accompanied by persistent functional abnormalities. Cutaneous anergy is a direct result of the viral effects on CD4 cells.
After acute infection and seroconversion, clinical latency may last several years before onset of symptoms due to development of secondary infection, malignancy, or neurologic disease. There is no biologic latency, however. HIV infection is a chronic, persistent infection of variable viral replication rate.
The viral load set point after acute infection correlates with rate of progression to symptomatic infection or AIDS. Several proprietary assays provide quantitative measurement of plasma HIV RNA. The branched (b)DNA assay detects as few as 20 to 50 copies per milliliter. Recognition of acute infection is important because early antiretroviral treatment may prevent extensive seeding of lymphoid tissues or even eliminate infection. Without treatment, viral replication is robust and even in the absence of a decline in CD4 count may cause cardiovascular disease, nephropathy, and non-AIDS-related cancers.
It is estimated that 10 billion virions enter the plasma daily in untreated people. Virus is found mainly in tissues, not plasma; total lymphoid viral burden is three times that of plasma, the majority in follicular dendritic cells within germinal centers, where virus is passively adherent. The total body viral load is 100 billion HIV RNA copies. Approximately 10% of latently infected cells contain replication-competent provirus. Cellular destruction of lymphoid tissue is mediated by direct HIV-cytopathic effects, autoimmunity, and other mechanisms. Eventually, the lymphoid system is overwhelmed by the viral burden, which increases with advancing disease and culminates in AIDS.
Other factors that may augment HIV replication and the onset of symptoms include the following: the biologic variability of HIV and the appearance of increasingly virulent strains; host immunogenetics; and interactions with concomitant infection by cytomegalovirus (CMV), herpes simplex virus, hepatitis B and C viruses, human herpesvirus (HHV)-6, and human T-lymphotropic virus type 1 (HTLV-1) that upregulate expression of HIV and cell-killing ability by cytokines. Cytokines and chemokines are released by immune cells in response to infection and may upregulate or downregulate viral replication.
Other immunologic abnormalities in AIDS are caused by effects of HIV on B cells or macrophages, which result in hypergammaglobulinemia, impaired antibody responses to new antigens (including encapsulated bacteria), and increased levels of immune complexes. Antibodies to platelets may cause thrombocytopenia.
cART and specific prophylaxis have reduced the incidence of AIDS-related opportunistic infections and neoplasms in the United States and other countries where treatment is readily available. cART refers to the use of three or more antiretroviral drugs from two antiretroviral drug classes. The major classes of antiretroviral drugs include nucleotide reverse transcriptase inhibitors, nonnucleotide reverse transcriptase inhibitors, protease inhibitors, integrase inhibitors, entry inhibitors, and fusion inhibitors. These antiretroviral drug classes interfere with different stages of HIV replication. The types of infections or neoplasms that complicate HIV infection have not changed and are similar worldwide, with varying frequencies depending on local factors. In untreated HIV infection, PCP is the most common opportunistic pathogen. Other opportunistic infections are often multiple and include fungal, viral, bacterial, and parasitic organisms. Many of these infections involve the CNS, usually secondarily but sometimes as the primary infection. For example, the papovavirus that causes progressive multifocal leukoencephalopathy causes a primary brain infection. Infections that are common in developing countries, such as trypanosomiasis, cysticercosis, and malaria, are sometimes seen in recent immigrants to the United States. Hepatitis B and C infections are important comorbid conditions, especially among those who acquire HIV from injection drug use. Kaposi sarcoma (an AIDS defining erythematous macular or nodular patch typically involving the face, oral mucosa, or upper trunk), Hodgkin and non-Hodgkin lymphoma, and cervical cancer, the most commonly encountered neoplasms related to immunosuppression, have become very rare in the setting of effective antiretroviral treatment. Non-AIDS-defining malignancies are now more common in treated populations, including anal cancer, lung cancer, liver cancer, and cancers of the head and neck. With the use of cART, HIV-positive individuals live significantly longer, and indeed more than 75% of HIV-positive individuals older than 50 years of age now die from non-HIV-related causes.
CENTRAL NERVOUS SYSTEM PATHOGENESIS
HIV enters the CNS at the time of primary infection and can result in no apparent disease, in acute self-limited syndromes, or in chronic disorders. Neurologic disorders are found in up to 70% of patients in clinical series, and more than 80% of autopsy series, of AIDS patients. In 10% to 20% of patients, the neurologic disorder is the first manifestation of AIDS. Uncommonly, a neurologic disorder is the sole evidence of chronic HIV infection and the cause of death. A high prevalence of neurologic disorders is observed in all populations studied, including those in sub-Saharan Africa and Asian regions bordering the Pacific Ocean. Despite the reduction in incidence of primary HIV-related syndromes, autopsy series of cART-treated patients who died of AIDS or unrelated causes show abnormalities in most brains, which in some cases were the cause of death. Cognitive impairment or HIV-associated neurocognitive disorder (HAND) is the most important HIV-related clinical syndrome.
Evidence of early CNS invasion includes isolation of virus from cerebrospinal fluid (CSF) or neural tissue (brain, spinal cord, peripheral nerve) and intrathecal production of antibodies to HIV. How HIV enters the CNS is not known. Possible mechanisms include intracellular transport across the blood-brain barrier within infected macrophages, as free-virus seeding of the leptomeninges, or as free virus after replication within the choroid plexus or vascular epithelium. In vitro studies using a proteomic platform suggest that HIV-1-infected monocyte-derived macrophages upregulate a large number of human brain microvascular endothelial cells, causing blood-brain barrier dysfunction that facilitates the development of CNS disease. Chemokines seem to play an important role in enhanced transmigration of HIV-infected lymphocytes across the blood-brain barrier. In vitro studies show enhanced HIV-infected leukocyte transmigration in response to the chemokine CCL2 (monocyte chemoattractant protein [MCP]-1) with disruption of the blood-brain barrier, enhanced permeability, reduction of tight junction proteins, and expression of the matrix metalloproteinases MMP-2 and MMP-9. In the brain, viral infection is detected only in microglial cells or macrophages by in situ hybridization techniques; it is not found in neurons or glial cells, even though these cells have CD4 and chemokine receptors.
The high frequency of neurologic disorders in HIV infection has led to the designation of HIV as a neurotropic virus. The term neurotropic implies selective vulnerability and targeting of brain by the virus. Alternatively, the high frequency of neurologic disorders may be explained by the chronicity of infection, which results in continued seeding of the CNS and chronic immune activation. Specific neurotropism is not needed for continued accrual of neurologic damage. It has been difficult to establish correlation of neurologic syndromes with productive viral replication in the affected tissue. There is, however, an increase in the viral burden or viral load with advancing disease that parallels dementia and other neurologic syndromes. The mechanism of neurologic injury is believed to be indirect. Potential mechanisms include immune-mediated indirect injury; restricted persistent cellular infection; cellular injury due to cytokines released by infected monocytes and macrophages; excitotoxic amino acid injury; voltage-mediated increase of intracellular calcium; free radical damage; potentiation of inflammatory damage by chemokines and lipid inflammatory mediators (arachidonic acid and platelet-activating factor); direct cellular toxicity of HIV gene products, such as the envelope gp120, tat, and gp41; and cross-reacting antibody to an HIV glycoprotein binding a cell membrane epitope, resulting in cell receptor blockade. Studies show the involvement of double-stranded RNA-activated protein kinase in apoptotic neuronal death due to HIV-gp120. This enzyme is elevated in brain tissue of patients with HIV dementia. More than one mechanism may be important. Genetic changes in the virus in the host may result in noncytopathic CNS virus with enhanced replicative capacity in monocytes and macrophages, leading to a greater viral burden in the CNS than is apparent in the periphery. Phenotypic and viral load discordance is documented in several studies of plasma and CSF.
This compartmentalization of virus may explain the occurrence of neurologic syndromes when peripheral viral replication appears to be well controlled.
CLINICAL MANIFESTATIONS
HIV-RELATED SYNDROMES
Neurologic disorders may occur at any stage from seroconversion to AIDS. Dementia and myelopathy are diagnostic of AIDS even without opportunistic infections; neuropathy is the most common direct HIV-related neurologic disease. All levels of the neuraxis may be affected, including multisystem disorders. Neurologic disorders are likely to be transient in early HIV infection, but they become progressive or chronic with persistent infection and worsening immunosuppression.
The neurologic syndromes in early HIV infection are indistinguishable from disorders that occur with infection by other viruses (Table 67.4). These include aseptic meningitis, reversible encephalopathy, leukoencephalitis, seizures, transverse myelitis, cranial and peripheral neuropathy (Bell palsy, Guillain-Barré syndrome), polymyositis, and myoglobinuria. Brachial neuritis and ganglioneuritis have been reported only rarely. The course is typically self-limited, and patients often experience full neurologic recovery. A recent study from the Multicenter AIDS Cohort Study suggests that older HIV-positive individuals in the cART era experience a higher incidence of neurologic disease compared to agematched HIV-negative individuals. In addition, HIV-positive individuals experience neurologic diagnoses at an earlier age compared to HIV-negative individuals. Excess neurologic disease was found in the categories of nervous system infections, dementia, seizures/epilepsy, and peripheral nervous system disorders in this study.
Acute inflammatory demyelinating polyneuropathy of the Guillain-Barré type
Polymyositis
Myoglobinuria
CSF abnormalities (pleocytosis up to 200 cells/mm3 and oligoclonal bands) differentiate HIV syndromes from postinfectious disorders. Tests for HIV antibody may be negative because these syndromes may precede or accompany seroconversion, and the tests must be repeated in several weeks. If acute HIV infection is strongly suspected, p24 antigen and viral load assay should be considered if serology is negative. Hepatitis B and hepatitis C serology should be determined in all HIV-seropositive patients. Early antiretroviral therapy may be offered to decrease the high viral load typical of acute infection quickly, thereby lowering the viral load set point. No specific treatment is indicated for these self-limited disorders except that plasmapheresis or immunoglobulin is used in cases of Guillain-Barré syndrome and steroids for polymyositis.
In chronic HIV infection, neurologic disorders may accompany systemic HIV disease or secondary disorders (Table 67.5).
Chronic or recurrent CSF pleocytosis sometimes occurs with meningeal symptoms but is often asymptomatic. Chronic pleocytosis does not predict any specific neurologic complication. Ascribing CSF pleocytosis to HIV infection requires exclusion of secondary pathogens or tumor. In a cross-sectional study, HIV-related CSF pleocytosis was uncommon in individuals with blood CD4 counts below 50 cells/µL or in those on effective antiretroviral therapy.
HIV-Associated Neurocognitive Disorder
Cognitive impairment is a well-recognized complication of chronic HIV infection in all populations; it can range from mild to severe (Table 67.6). Its prevalence may be underestimated in resource-limited settings. Despite some success, there are enormous challenges to developing special dementia scales for use in resource-limited settings, including multiple languages, regional dialects, and low formal education rates. The International HIV Dementia Scale is a brief screening test that can be performed by nonneurologists and has been validated as a potential screening test for dementia in HIV-positive individuals in resource-limited settings. There are several scales for classification of HIV cognitive impairment, including revision of the AIDS Task Force of the American Academy of Neurology (AAN) criteria.
Persistent or recurrent meningeal pleocytosis with or without meningeal symptoms
Diffuse and focal cerebral syndromes
Dementia, static or progressive with or without motor signs
Mild cognitive impairment, neuropsychological test criteria only
Organic psychiatric disorder
Cerebrovascular syndromes
Cerebellar ataxia
Seizure disorder
Multisystem degeneration
Chronic progressive myelopathy
Cranial and peripheral neuropathies
Bell palsy
Hearing loss
Phrenic nerve paralysis
Lateral femoral cutaneous nerve
Chronic inflammatory demyelinating polyneuropathy
Distal symmetric sensory neuropathy
Mononeuritis multiplex
Autonomic neuropathy
Myopathy
Minor motor signs, usually motor slowness or tremor, may be present. HIV-associated dementia, known variously as HIV-1-associated dementia complex,HIV dementia, or AIDS dementia complex, is diagnostic of AIDS. Older designations are subacute encephalitis, subacute encephalopathy, or HIV encephalitis. HIV dementia refers to HIV-positive individuals with moderate to severe cognitive impairment on neuropsychological testing and marked difficulties in activities of daily living due to the cognitive impairment. In the pre-cART era, HIV dementia, the most severe stage of HAND, was a common stage of cognitive impairment among HIV-positive individuals with advanced immunosuppression. In HIV-positive individuals on cART, HIV dementia is rarely seen, and less severe stages of HAND such as HIV-associated mild neurocognitive disorder (MND) are the most common clinically recognized stage of cognitive impairment. HAND including all three stages (asymptomatic neuropsychological impairment [ANI], MND, and HIV dementia) may be seen in 40% to 50% of HIV-positive individuals with advanced infection in some studies, with ANI and MND being the most common stages. Peripheral neuropathy coexists in 25% of patients.
HIV dementia in the absence of cART is an insidiously progressive subcortical dementia. Early symptoms include apathy, social withdrawal, diminished libido, slow thinking, poor concentration, and forgetfulness. Psychiatric syndromes, such as psychosis, depression, or mania, are sometimes profound and may be the first manifestation of HIV infection. Motor signs include slow movements, tremor, parkinsonian features, leg weakness, and gait ataxia. There may also be headaches, seizures, or frontal release signs. Although the disorder is usually progressive in HIV-positive individuals not on cART, some patients on cART develop a static level of disability, and others may improve in response to medical treatment for HIV or complicating disorders. When progressive, the disease culminates in akinetic mutism, an immobile bedridden state with global cognitive impairment and urinary incontinence.
In children, there may be a similar static or progressive encephalopathy. Most affected children meet criteria for AIDS, but progressive encephalopathy can occur before immunologic dysfunction is severe. Neurologic findings include intellectual deterioration, microcephaly, loss of developmental milestones, and progressive motor impairment that may culminate in spastic quadriparesis and pseudobulbar palsy. Seizures are usually due to fever. Myoclonus and extrapyramidal rigidity are rare.
The CSF is usually normal or shows mild pleocytosis, protein elevation, and oligoclonal bands. Virus can be cultured from CSF. In HIV-positive individuals not on cART, both CSF and plasma viral load correlate with occurrence of dementia but may be discordant in some cases where CSF load is greater than plasma. In HIV-positive individuals on cART, CSF and plasma viral load do not correlate with HAND stage. CSF markers of immune activation, HIV p24 antigen, β2-microglobulin, tumor necrosis factor, and antimyelin basic protein in cART-treated HIV-positive individuals do not correlate with severity of dementia. None of these markers is predictive of, or specific for, dementia. CSF and serum markers such as neopterin and tryptophan levels and CSF serotonin metabolites and quinolinic acid levels lack predictive value or specificity but can correlate with severity of dementia. Elevated levels of CSF neurofilament protein, a marker of axonal injury, are found in HIV-infected patients with dementia. Levels decline in individuals who have a clinical response to antiretroviral therapy, suggesting its possible use as an indicator of drug efficacy. Efforts to identify markers for progression to dementia have been disappointing. A recent study suggested that increased levels of sphingomyelin and ceramide and the accumulation of lipid peroxidation products are associated with declining cognitive status. Further studies are needed to confirm these findings.
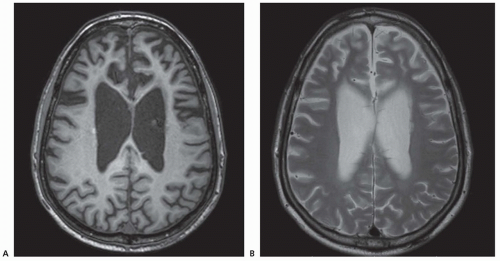
FIGURE 67.1 HIV-positive subject with progressive dementia. A: T1-weighted and (B) T2-weighted MRI scans show ventricular enlargement and cortical atrophy, particularly in the frontal lobe. There is also some mild periventricular T2 hyperintensity.
In adults, computed tomography (CT) or magnetic resonance imaging (MRI) scans show cortical atrophy and ventricular dilatation, sometimes with white matter changes. On CT, there is attenuation of white matter; MRI shows hyperintense white matter lesions on T2-weighted and proton density sequences ranging from discrete foci to large confluent periventricular lesions (Fig. 67.1).
CT in children shows basal ganglia calcification and cerebral atrophy. MRI white matter changes may not correlate with dementia and may disappear spontaneously or with antiretroviral therapy.
Abnormalities in functional neuroimaging are detected in HIV-infected individuals whether they have dementia or not. The abnormalities become worse or change with progressive cognitive impairment. 18F-fluorodeoxyglucose-positron emission tomography (PET) shows relative hypermetabolism in the thalamus and basal ganglia in HIV-infected individuals. Progressive dementia is accompanied by cortical and subcortical hypometabolism. Singlephoton emission computed tomography (SPECT) shows multifocal cortical perfusion deficits in the frontal lobes, worse in those with dementia. Cerebral metabolite abnormalities demonstrated by magnetic resonance spectroscopy (MRS) include elevated myoinositol and choline levels in frontal white matter indicative of glial proliferation in patients with mild cognitive impairment. Severe dementia is associated with decreased levels of N-acetylaspartate, a neuronal marker. Dynamic cerebral blood volume (CBV) studies by functional MRI show increased CBV in deep and cortical gray matter in HIV-positive individuals and even greater increases in the deep gray matter of those with dementia. Continuous arterial spin label MRI showed reduced caudate blood flow and volume in patients with cognitive impairment. Abnormalities may improve with antiretroviral treatment.
Pathologic abnormalities in brain include microglial nodules, multinucleated giant cells, focal perivascular demyelination and gliosis, and neuronal loss in frontal cortex. Although there is often no correlation between the severity of these pathologic changes and the severity of dementia, recent studies suggest that neuronal injury may be missed by standard pathologic survey techniques. In a prospective study, severity of neurocognitive impairment was correlated with microneuroanatomic injury to dendritic structures that resulted in dendritic simplification but not to viral burden or presence of microglial nodules and multinucleated giant cells. Astrocyte cell death through apoptotic mechanisms may reduce the neuroprotective functions of this cellular population. In vitro studies show that soluble Fas ligand (sFasL) from HIV-infected macrophages triggers apoptosis of uninfected astrocytes. A study of pre-cART HIV-infected patients with dementia showed elevated CSF sFasL levels in this group compared with HIV-negative controls and HIV-positive nondemented patients. More prospective data are needed to understand the role of apoptosis in HIV dementia and the use of markers for apoptosis as predictors of dementia.
The incidence of HIV dementia is lower than the frequency with which pathologic abnormalities are found. The CDC reported a prevalence of 7.3% for the diagnosis of HIV encephalopathy in 1987 through 1991. The Multicenter AIDS Cohort Study Group reported a 4% prevalence of dementia diagnosis, with a 7% annual rate and 15% overall probability of dementia before death. There are increased mortality rates among demented patients. A subset of individuals may show clinical progression in their HAND stage. Some HIV-positive individuals on cART may demonstrate ongoing CNS changes as identified by subcortical atrophy on MRI studies in the absence of clinical changes. Other HIV-positive individuals may show clinical deterioration on neuropsychological testing. Some HIV-positive individuals may show clinical improvement which is sustained. Additional HIV-positive individuals with HAND may have a fluctuating course from abnormal to normal and then abnormal neuropsychological test performance again. HIV dementia now is rarely seen in the United States where cART is commonly used. However, in resource-limited countries, many HIV-positive individuals are not on cART. In 2012, according to UNAIDS, around 9.7 million people living with HIV infection had access to antiretroviral therapy in low- and middle-income countries. This number represents 61% of people eligible for treatment under the 2010 WHO guidelines and only 34% of people eligible under the 2013 WHO guidelines. In sub-Saharan Africa, where 70% of the world’s HIV-positive population resides because HIV-positive individuals are frequently not on cART, the frequency of HIV dementia may be much higher than the prevalence in the United States. Studies in Uganda suggest that the frequency of HIV dementia among antiretroviral-naïve HIV-positive individuals presenting to an infectious disease clinic may be as high as 31% to 41%. If this proportion is seen throughout resource-limited countries, then HIV dementia may be among the most common forms of dementia globally along with Alzheimer disease and vascular dementia. The question of whether specific HIV subtypes are associated with an increased risk of dementia is unresolved, with some studies showing an increased risk for dementia in HIV subtype D-infected individuals compared to HIV subtype A-infected individuals in Uganda, whereas other studies show no association of HIV subtype with risk of dementia. Similarly, initial studies suggested that HIV subtype C may have a decreased risk of dementia compared to subtype B, but recent studies suggest no difference between HIV subtypes B and C and risk of dementia.
The diagnosis of HIV-associated dementia requires exclusion of secondary opportunistic infections or neoplasms. Other confounding variables include drug use, vitamin B12 deficiency, metabolic disorders, concurrent infections such as hepatitis C infection, CNS side effects of medications (e.g., efavirenz, which can cause CNS side effects in 50% of HIV-positive individuals after initiation), and age-related comorbidities in an aging HIV-infected population due to successful antiretroviral treatment. Older survivors of HIV are at risk for vascular disease and degenerative disorders associated with dementia such as Alzheimer disease. In most studies, antiretroviral therapy reduces the incidence and mortality of AIDS dementia. In general, the prevalence of HAND in HIV is expected to increase with longer survival and the aging of HIV-positive individuals. The primary treatment for HAND is cART, which is associated with cognitive improvement in the majority of antiretroviral-naïve HIV-positive individuals. Treatment of comorbid conditions frequently associated with HAND such as depression is also beneficial. Clinical trials of adjunctive therapies such as selegiline, a monoamine oxidase type B inhibitor, and minocycline have showed no benefit. Antioxidants and agents that block gp120 are ineffective. Neuropsychological test abnormalities can accrue with advancing disease. Those showing a decline in neuropsychological test performance, however, have an increased risk of death. In an early multicenter study of 19,462 HIV-infected people, the strongest predictors of significant dementia were CD4+ T-lymphocyte counts of less than 100 cells/µL, anemia, and an AIDS-defining infection or neoplasm (18.6% to 24.9% risk in 2 years). In the post-highly active antiretroviral therapy (HAART) era, HAND is often independent of advanced immunosuppression.
Antiretroviral therapy using drugs with good CNS penetration may benefit the symptomatic patient with CNS virologic escape, but some studies suggest that the beneficial effect of treatment is independent of CNS penetration. A randomized clinical trial of cART with good CNS penetration compared to cART with poor CNS penetration showed no clinical benefit for the group randomized to cART with good CNS penetration. Suppression of viral replication in both the blood and CSF is critical for effective treatment of HAND. Initiation of cART is usually associated with immune system recovery and cognitive benefits. However, some HIV-positive individuals after initiation of cART may experience clinical deterioration despite recovery of the immune system from immunodeficiency, a condition known as immune reconstitution inflammatory syndrome (IRIS). When IRIS involves the CNS, opportunistic infections of the CNS such as cryptococcal meningitis or progressive multifocal leukoencephalopathy may present. In addition, an acute syndrome of fulminant HIV encephalitis can occur in rare cases in which cognition worsens despite virologic suppression and immune system recovery. Risk factors for IRIS include a low CD4 nadir at initiation of cART, the presence of an underlying opportunistic infection, and a sharp decline in viral load after starting cART. Corticosteroids have been used in HIV-positive individuals with noninfectious encephalitis after cART initiation, with clinical improvement in some cases. Additional studies of the role of corticosteroids for the treatment of IRIS are needed.
Only gold members can continue reading. Log In or Register to continue