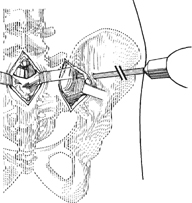
41 Paul T. Rubery and John T. Gorczyca A bar or rod placed transversely through the posterior iliac tubercles, posterior to the sacrum, can serve as a safe and reliable distal anchor for complex instrumentation constructs across the lumbosacral junction. Force concentration at the junction of the relatively mobile lumbar spine with the relatively immobile pelvis is a significant cause of spinal instrumentation failures. The relatively poor bone stock of the sacrum compromises pedicle screw fixation. Additional anchor points enhance fixation and may decrease the incidence of instrumentation failure and pseudarthrosis. This technique provides additional, extraspinal fixation into relatively strong bone. Instrumentation constructs extending proximal to L2 and crossing the lumbosacral junction. The technique can be applied in clinical situations involving particularly high-grade instability at L5-S1, as well as pseudar-throses of previous L5-S1 fusions. Deficiency or absence of posterior iliac bone precludes rod placement. A preoperative computed tomography (CT) scan of the pelvis is useful to assess the adequacy of the ilium for passing the transiliac rod. Specially manufactured connectors may be required to join the transversely oriented transiliac rod to the longitudinal member of the spinal instrumentation. The surgeon should carefully position the patient’s hips to preserve or reconstruct the normal sagittal contours of the spine. With the patient in the prone position, using a midline skin incision, the sacrum is exposed out to the ala bilaterally. Separate vertical incisions are made lateral to the palpable posterior-superior iliac spines (PSISs), and their lateral aspects are exposed. A rod insertion site is identified. This is approximately 2 cm anterior to the PSIS, and positioned to allow transverse rod placement dorsal to the sacrum. An appropriate trocar-tipped threaded rod is chosen, mounted on a hand drill, and using an additional laterally placed stab incision, the rod is driven through the ilium, and toward the contralateral side (Fig. 41.1). The surgeon must take care to ensure that the advancing rod remains dorsal to the sacroiliac (SI) joint and the sacrum, and also ensure that any connectors are placed on the transverse rod before engaging the opposite ilium. As the rod emerges at the opposite ilium, it can be cut to length with a rod cutter, and nuts or locking washers applied to prevent disengagement from the bone. Coupling the rod to the longitudinal members completes the construct (Fig. 41.2).
Iliosacral Screw Fixation Techniques
Transiliac Rod Placement
Description
Key Principles
Expectations
Indications
Contraindications
Special Considerations
Special Instructions, Position, and Anesthesia
Tips, Pearls, and Lessons Learned
Difficulties Encountered
Key Procedural Steps
Related posts:
 Lateral Extracavitary Approach
Open Reduction of Unilateral and Bilateral Facet Dislocations
Thoracoplasty: Anterior, Posterior
Thoracic Pedicle Screw Placement: Anatomic, Straightforward, and In-Out-In Techniques
Closed Cervical Traction Reduction Techniques
Rib Expansion Technique for Congenital Scoliosis
Lateral Extracavitary Approach
Open Reduction of Unilateral and Bilateral Facet Dislocations
Thoracoplasty: Anterior, Posterior
Thoracic Pedicle Screw Placement: Anatomic, Straightforward, and In-Out-In Techniques
Closed Cervical Traction Reduction Techniques
Rib Expansion Technique for Congenital Scoliosis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


