21
Odontoid Screw Placement
Darrel S. Brodke
Description
Reduction and fixation of a type II or high type III odontoid fracture with a precisely placed lag/compression screw.
Key Principles
Anatomic alignment at the fracture site by initial positioning or intraoperative reduction is vital to the success of this procedure. The lag screw must be able to glide through the vertebral body and firmly purchase the odontoid fragment to gain firm compression at the fracture edges.
Expectations
Screw fixation of the odontoid fracture should significantly improve fracture-healing rates over those treated in halo-vest immobilization, and avoid the limitations of a primary C1-C2 fusion, with associated loss of motion.
Indications
Patients with acute or subacute (less than 6 months old) type II or high type III odontoid fractures, particularly those at higher risk of pseudarthrosis, are ideal for this technique.
Contraindications
- Fractures older than 6 months
- Reverse (anterior) oblique fracture line, angling from posterior rostral to anterior caudal (Fig. 21.1)
- Significant osteoporosis or fracture comminution
- Inability to gain anatomic reduction
- Inability to gain appropriate screw placement, due to body habitus (barrel chest) or associated disease process (ankylosing spondylitis)
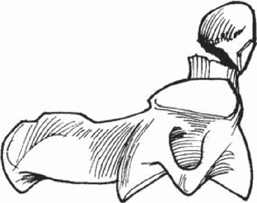
Fig. 21.1 A reverse (anterior) oblique fracture, not amenable to odontoid screw fixation.
Special Considerations
Patients older than 50 years of age, with fractures displaced greater than 4 to 5 mm, have the highest rate of nonunion with halo fixation. They should be considered for immediate odontoid screw fixation. Likewise, younger patients with high-risk lifestyles and elderly patients who may poorly tolerate 3 months in a halo vest may be considered for immediate fixation. Those patients who do undergo 3 months in a halo and have persistent motion at the fracture site may still heal with screw fixation. Although there is often some loss of motion following odontoid fracture treatment by any means, the motion remains better than with C1-C2 fusion, which is associated with a 50% loss of rotation of the neck.
Special Instructions, Position, and Anesthesia
The patient should be positioned supine on the operating table with the head in traction. This can be accomplished with the Mayfield three-pin head-holder, Gardner-Wells tongs, and a pad under the head and between the shoulder blades, or with halter traction. The arms may be gently taped down to the sides with mild traction, though the shoulders rarely block visualization. If the endotracheal tube can be positioned off to the side in the mouth, this will allow improved visualization of the odontoid in the anteroposterior (AP) plane.
Tips, Pearls, and Lessons Learned
- Get as close to anatomic reduction as possible prior to the prep and drape. This can be accomplished by adjusting the height of the head on towels or foam, or by placing towels under the shoulder blades. Both rotation of the neck and forward translation of the head, as compared with the chest, may be required to reduce the fracture and allow access for screw placement.
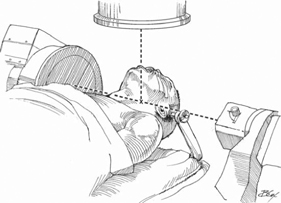
- Use biplane fluoroscopy to obtain quick AP and lateral views of the odontoid throughout the procedure (Fig. 21.2). A bight block, wad of gauze, or a wine cork with cutouts for the teeth may be used to hold open the mouth, improving AP visualization.
- Ensure access to the screw trajectory above the chest, and confirm on the lateral fluoroscopy view prior to prep and drape (Fig. 21.3).
- Approach through a C5-C6 level skin incision (on the right for a right-handed surgeon).
- Enter the C2 body at the C2-C3 disk, under the anterior edge of the body. This may require removing a small amount of the C3 body anteriorly, as well as some of the C2-C3 disk annulus, to get the correct trajectory.
- Further reduction may be achieved by using a radiolucent retractor that also enables the assistant to place anterior to posterior pressure on either the C2 vertebral body or the odontoid fragment.
Related posts:
 Anterior Thoracic and Thoracolumbar Plating Techniques
Anterior Thoracic and Thoracolumbar Plating Techniques
 Reduction Techniques for Atlantoaxial Rotary Subluxation
Reduction Techniques for Atlantoaxial Rotary Subluxation
 Posterior Spinal Anchor Strategy Placement and Rod Reduction Techniques: Posterior (Rotation vs. In-Situ Translation)
Posterior Spinal Anchor Strategy Placement and Rod Reduction Techniques: Posterior (Rotation vs. In-Situ Translation)
 Iliosacral Screw Fixation Techniques
Iliosacral Screw Fixation Techniques
 Open Lumbar Microscopic Diskectomy
Open Lumbar Microscopic Diskectomy
 Spondylolysis Repair (Pars Interarticularis Repair)
Spondylolysis Repair (Pars Interarticularis Repair)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


