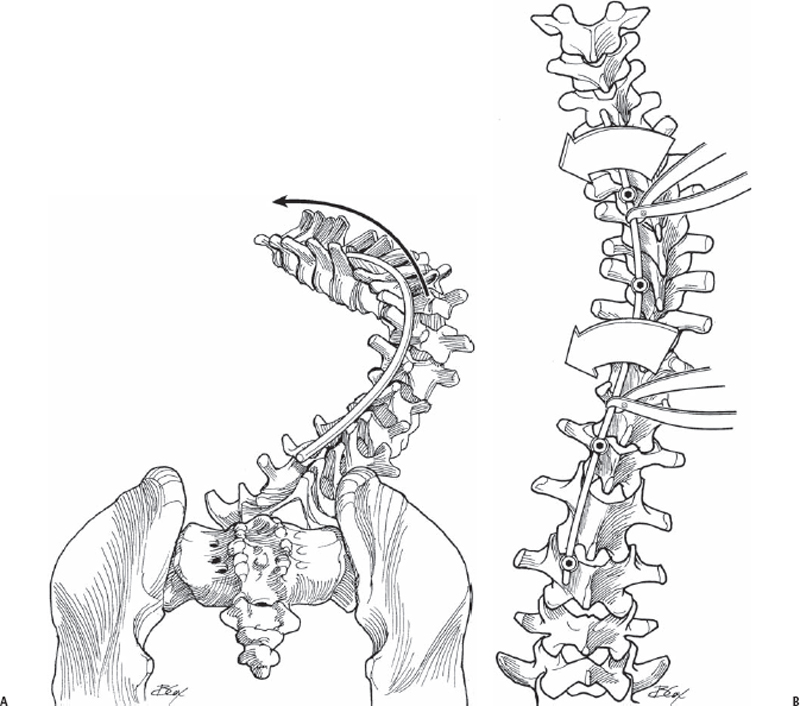
57 Fernando E. Silva and Lawrence G. Lenke Correction of scoliosis by posterior instrumentation using rotation versus in-situ translation techniques. A 90-degree counterclockwise rod-rotation maneuver permits correction of coronal and sagittal plane deformities in right thoracic scoliosis with hypokyphosis. This type of rod-rotation maneuver mostly translates the spine, in contrast to a true apical derotation maneuver using pedicle screw constructs. Translatory maneuvers via in-situ lateral bending loads can correct essentially all Lenke curve types, not just those hypokyphotic Lenke type 1 curves. Both techniques can be employed using hooks or screws. We recommend screws whenever possible, however, especially with large curves. Also, screws have the added advantage of possibly obviating the need of a thoracoplasty. Both types of corrective maneuvers should lead to a balanced spine. All Lenke curve types. With curves other than Lenke 1A (-) and 1A (N), the technique of a 90-degree counterclockwise rod-rotation maneuver should not be employed, especially with curves that are at risk for decompensation with a full rod-rotation maneuver. Relative contraindications for a posterior approach are Lenke type 5C curves, where an anterior approach is preferred in an attempt to prevent adjacent segment junctional kyphosis, if this curve type is approached posteriorly. Upright lateral radiographs are required to demonstrate mild lordosis or hypokyphosis in the thoracic profile (T5–T12). Always try to assess the curve to see if selective fusion can be performed, especially when dealing with Lenke 1-3C and 6C curves. Again, in the latter, in-situ translatory loads are recommended, along with apical derotation (as needed) and selective compression/distraction to obtain final spinal balance. Prone on Jackson frame or appropriate four-poster frame, ensuring adequate lumbar lordosis. The arms are placed in the 90–90 position. Neurologic monitoring equipment, with or without the Stagnara wake-up test, is deemed appropriate. In placing pedicle hooks, be sure not to break the superior facet so that the hook does not migrate ventrally, possibly offending the neural elements. In using free-hand placement of thoracic pedicle screws, each level should be instrumented in the same sequential manner. The technique is equivalent for lumbar and thoracic screws. It is imperative to clearly expose the base of the corresponding superior facet to serve as a guide to the imaginary location of the ventral pedicle. Do not force the Lenke probe into the pedicle. Once cancellous bone in the pedicle has been entered, the probe is easily inserted into the pedicle with a twisting and gentle pushing motion. All implants, hooks, or screws must be well positioned and constantly checked for any plowing (screws) or pull-out (screws and hooks). A derotation maneuver might prove difficult when addressing stiffer curves, and may lead to bone-implant failure, especially with hooks. In this situation, using an all-pedicle screw construct with in-situ translation corrective loads can circumvent the difficulty. When pedicles are very small or more than one pass has been made while placing pedicle screws, a Kirschner wire (K-wire) can be used for assistance, but only when it is absolutely certain that the bony floor of the pedicle tract is intact.
Posterior Spinal Anchor Strategy Placement and Rod Reduction Techniques: Posterior (Rotation vs. In-Situ Translation)
Description
Key Principles
Expectations
Indications
Contraindications
Special Considerations
Special Instructions, Position, and Anesthesia
Tips, Pearls, and Lessons Learned
Difficulties Encountered
Key Procedural Steps
Rod Rotation Maneuver (Figs. 57.1 and 57.2)
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


